

The Department of Spondylosurgery of the 1st Medical Faculty of Charles University and the Motol University Hospital is a specialized workplace dealing with spine surgery. The Department of Spondylosurgery of the 1st Medical Faculty of Charles University and the Motol University Hospital are among the leading centers in the Czech Republic in terms of the number of procedures performed and the scope of care provided.
The subject of her interest are practically all diseases of the spine: spinal cord injuries, degenerative diseases, cancer, spinal inflammations, congenital deformities.
The clinic makes full use of the unique possibilities of the Motol hospital, interdisciplinary cooperation of all experts in the care of patients with spinal diseases, starting with modern diagnostic methods and ending with specialized care for patients with spinal cord injuries.
The clinic provides care for injuries and emergencies 24 hours a day through a counseling system. He also performs continuous superconsulting activities for a number of district and smaller hospitals.
At our clinic, we perform almost every year 1400 spine surgery, around 12 000 patients is treated on an outpatient basis and 1600 patients hospitalized.

Prof. MUDr. Jan Stulik CSc.
Secretariat
(224) 432 581
Head of the clinic
Prof. MD Jan Štulík, CSc.
Tel .: 224432580, 2581
Email: jan.stulik@fnmotol.cz

Deputy head for medical and preventive activities
as. MD Jan Kryl
Tel .: 224432580, 2581
Email: jan.kryl@fnmotol.cz
Chief doctors
Standard department
as. MUDr. Tomas Vyskocil
Tel .: 224432573, 2572
Email: tomas.vyskocil@fnmotol.cz
Jip
as. MD Michal Barna
Tel .: 224432589, 2590
Email: michal.barna@fnmotol.cz
Doctors of spondylosurgery clinic
prof. MUDr. Zdenek Klezl, CSc.
Tel .: 224432574, 2599
MD Gábor Geri
Tel .: 224432589, 2590
MD Filip Pivarči
Tel .: 224432589, 2590
MD Lucie Salavcová
Tel .: 224432573, 2599
MD Michaela Rybárová
Tel .: 224432573, 2599
MD Michal Varga
Tel .: 224432573, 2599
MD Richard Hajduk
Tel .: 224432573, 2599
MD Jan Zemanek
Tel .: 224432573, 2599
MD Eva Vaskova
Neurologist, Center for Conservative Therapy (CKT FNM)
Phone: 224432575
Head nurse
Bc. Lenka Šipulová
Phone: No. 224 432 585
Email: lenka.sipulova@fnmotol.cz
Station ICU
Bc. Markéta Šimová
Tel: 224 432 2590
Email: marketa.simova@fnmotol.cz
Station nurse standard
Irena Kroupová
Phone: 224 432 570, 2573
Email: irena.kroupova@fnmotol.cz
Ambulance station nurse
Eliška Akachi
Tel: 224 432 592
Email: eliska.akachi@fnmotol.cz
The clinic specializes in surgical care for patients with spinal diseases.
Its basic task is a surgical solution spine injury with the subsequent primary phase of rehabilitation of these patients. They also fall into this area conditions after spinal injuries such as kyphotization or stabilization failure. Especially with emphasis on traumatology of the cervical spine, including injuries of the cervico-cranial junction. At present, the task of the department is also the follow-up care of patients with spinal cord injuries until the time of transfer to the rehabilitation workplace - Spinal Unit of the Motol University Hospital.
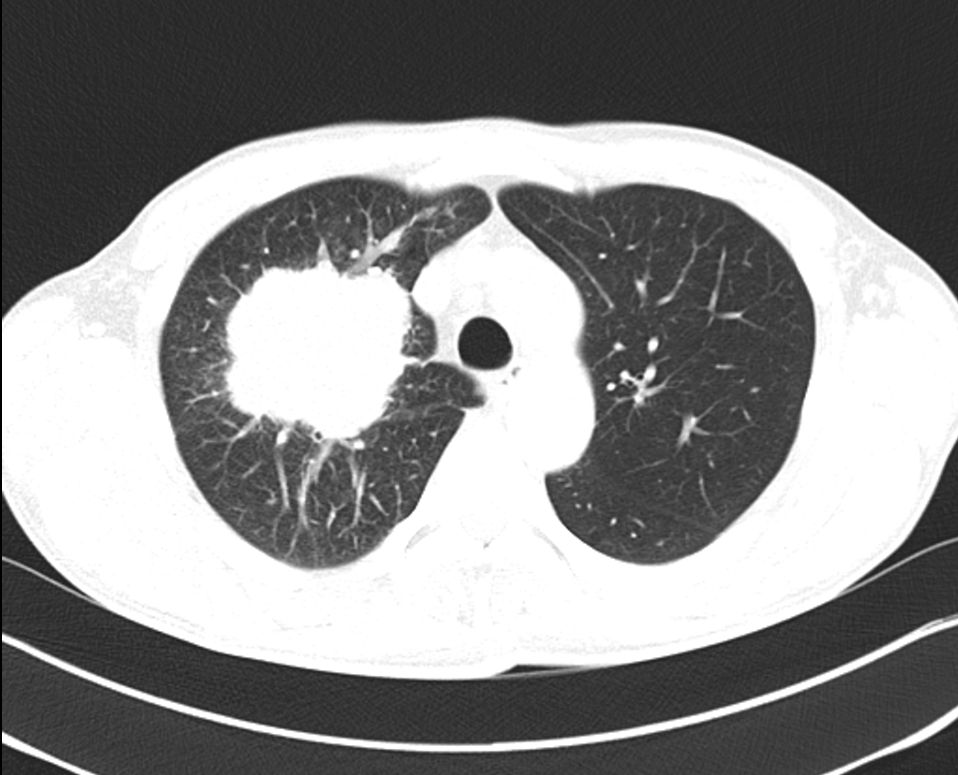
The clinic also takes care of patients with spinal cancer. This is the primary cancer illnesses and in particular o metastatic disabilities and pathological fractures with oppression of nerve structures, mostly accompanied by neurological deficits.
Another diseases belonging to the spectrum of care of spondylosurgery clinics are inflammation of the spine. They are also an integral part of spinal surgery degenerative diseases spondylosis, spondylarthrosis with cervical and lumbar spine stenosis, degenerative scoliosis, spondylolisthesis, instability. An important part is the surgical treatment of degenerative changes in the cervical spine in rheumatoid arthritis and congenital malformations.
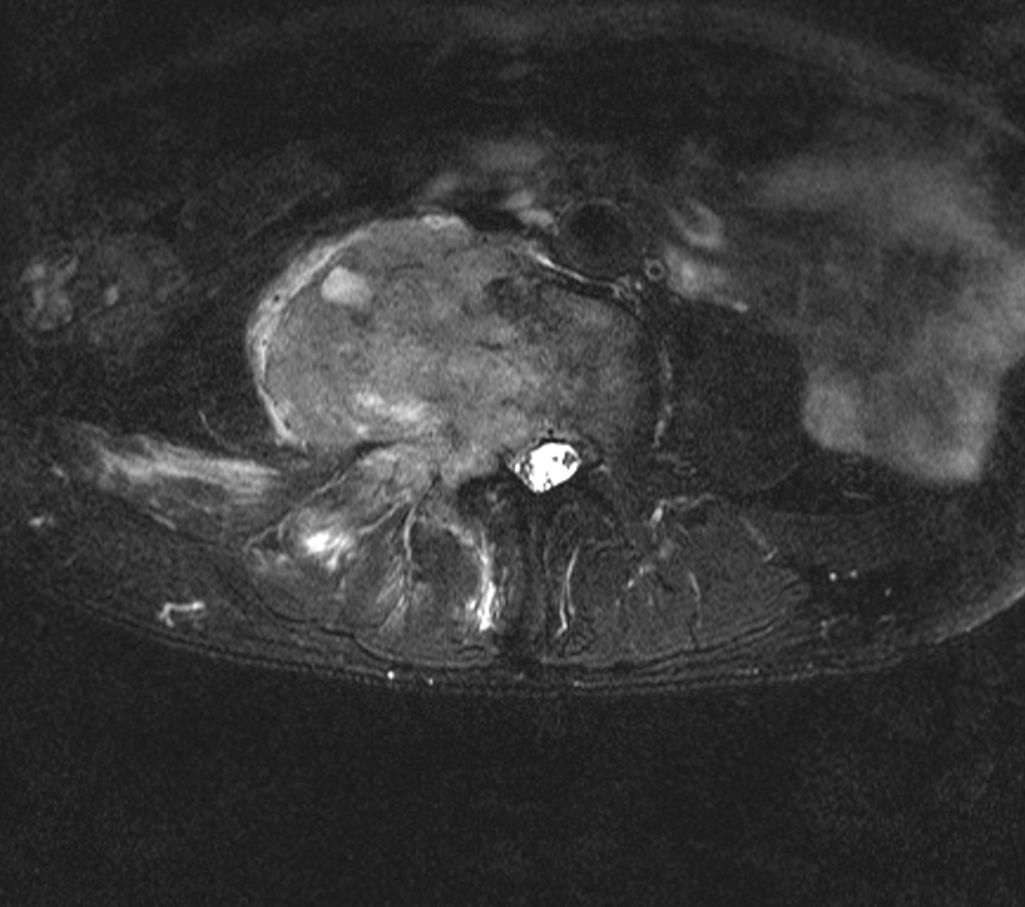
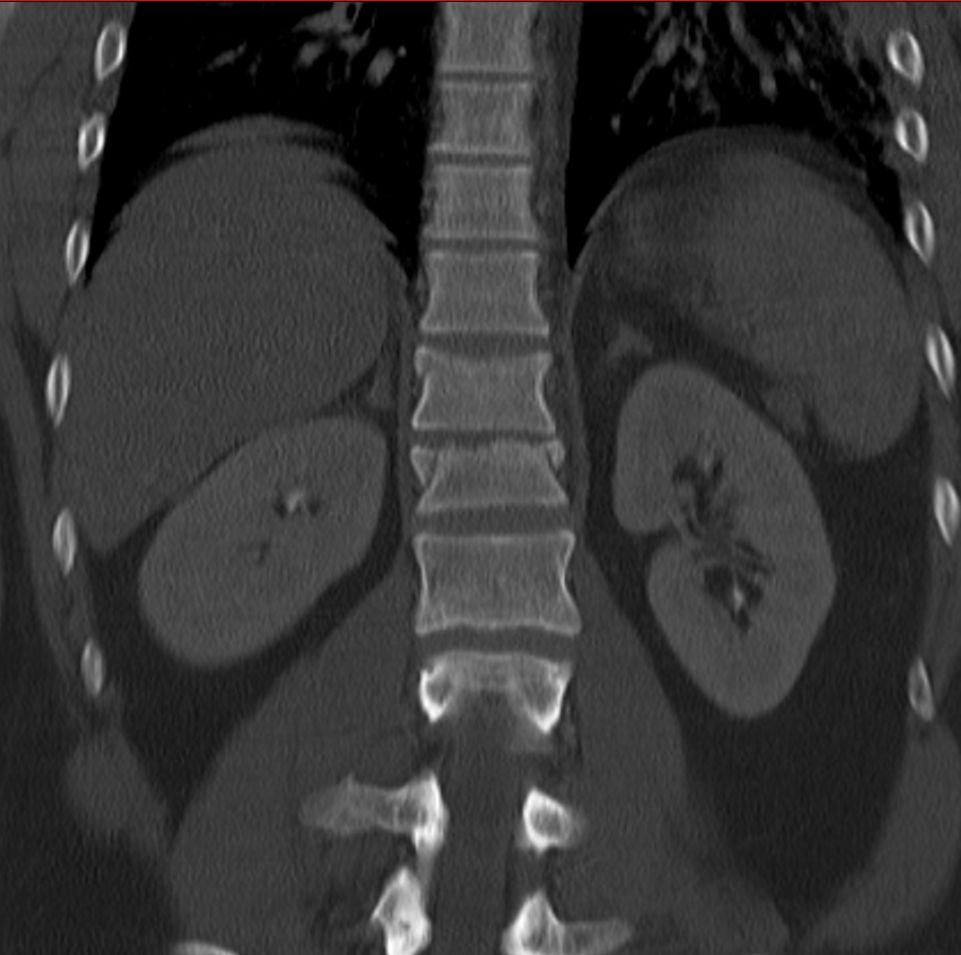
An example of surgical treatment of lumbar spine cancer.
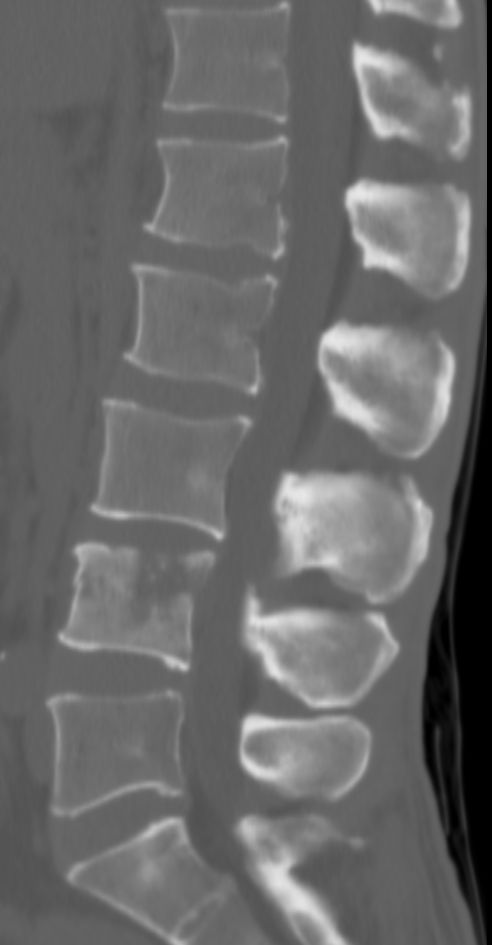




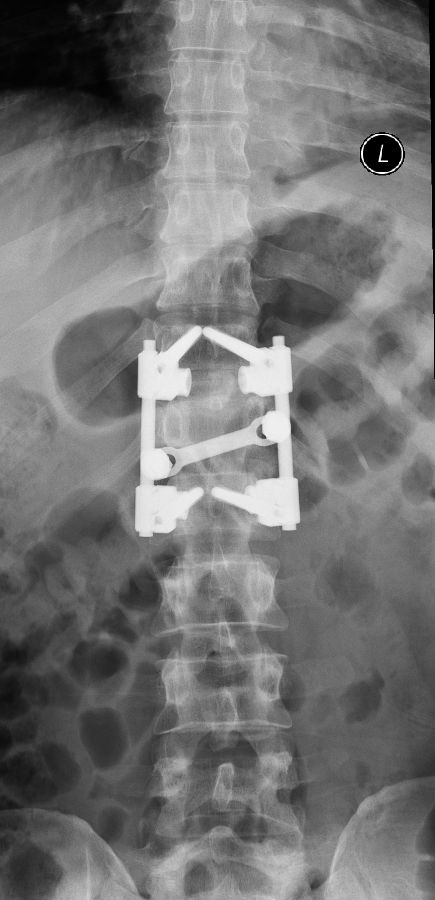
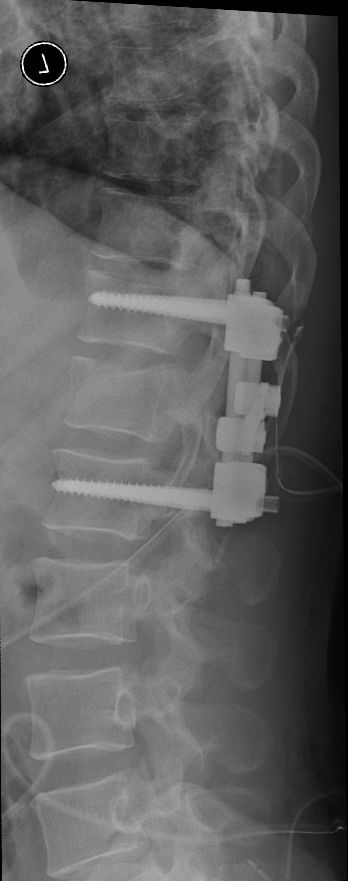
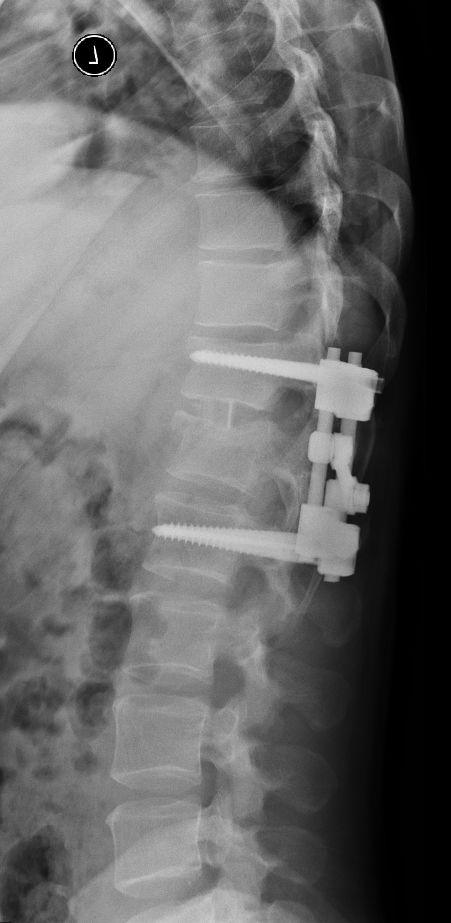
Example of surgical treatment of thoracic spine injuries. Patient with a dislocated fracture of the 12th thoracic vertebra (fr. T12) after falling from above. Primarily posterior position correction with removal of oppression of nerve structures, fixation with an internal transpedicular fixator to the vertebrae above and below the injured floor, including removal of bone grafts from the hip shovel and application of these grafts around the internal fixator (Socon Ti T11-L1, posterior desgraft grafts). Subsequently, in the second period, the replacement of the intervertebral disc between the 11th and 12th thoracic vertebra (T11-T12 discectomy) with a bone graft from the scapula of the hip bone.






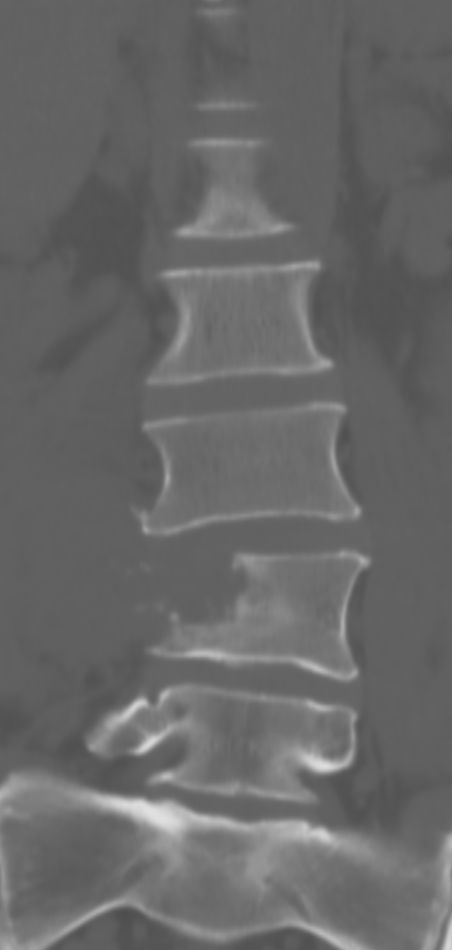
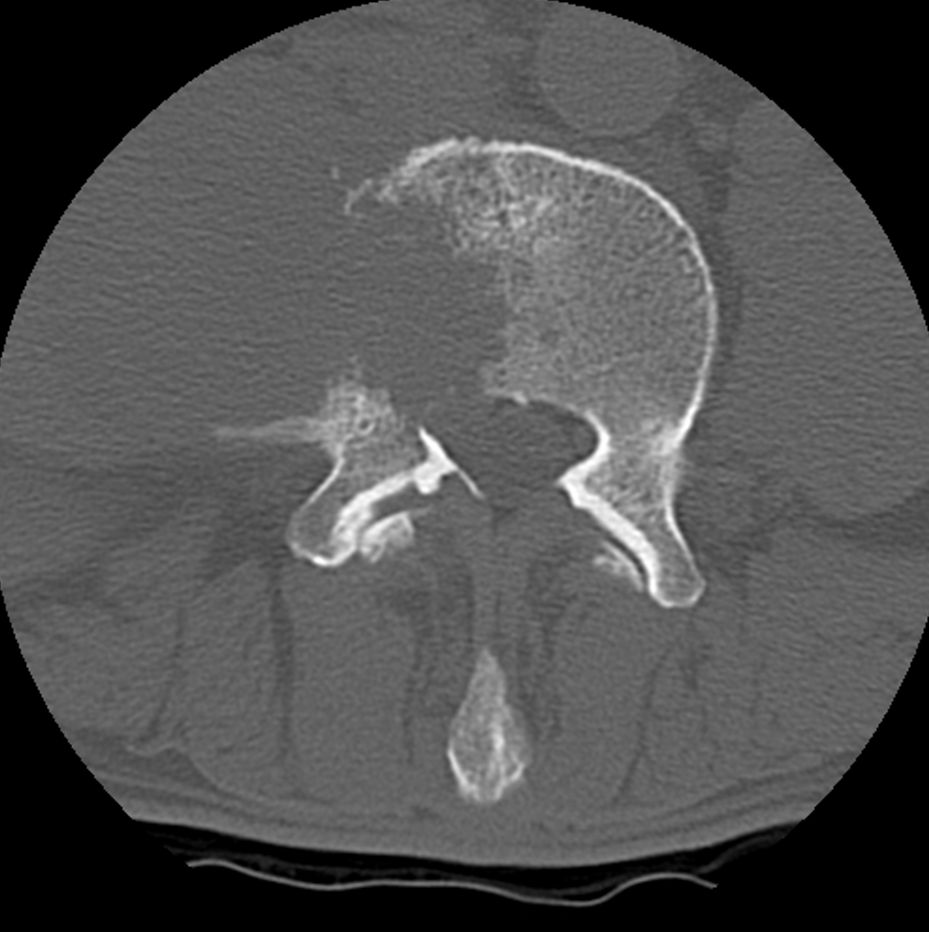
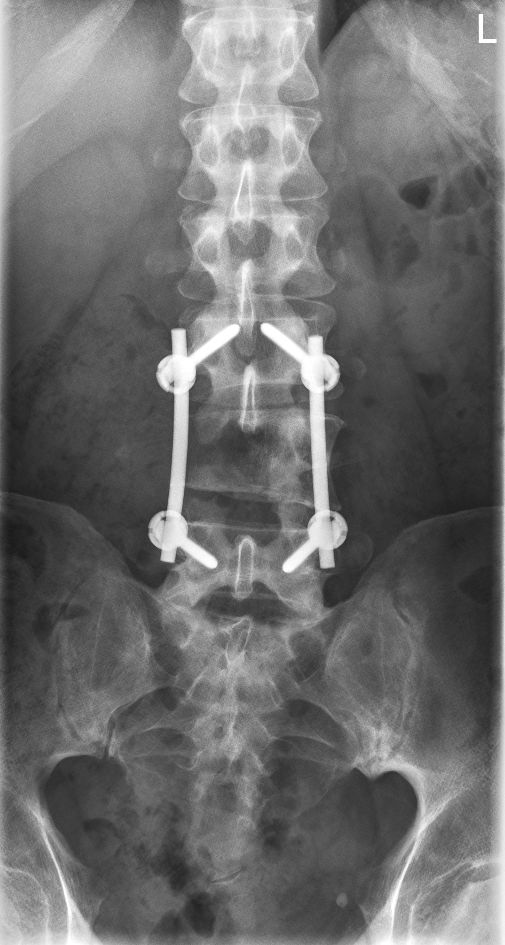
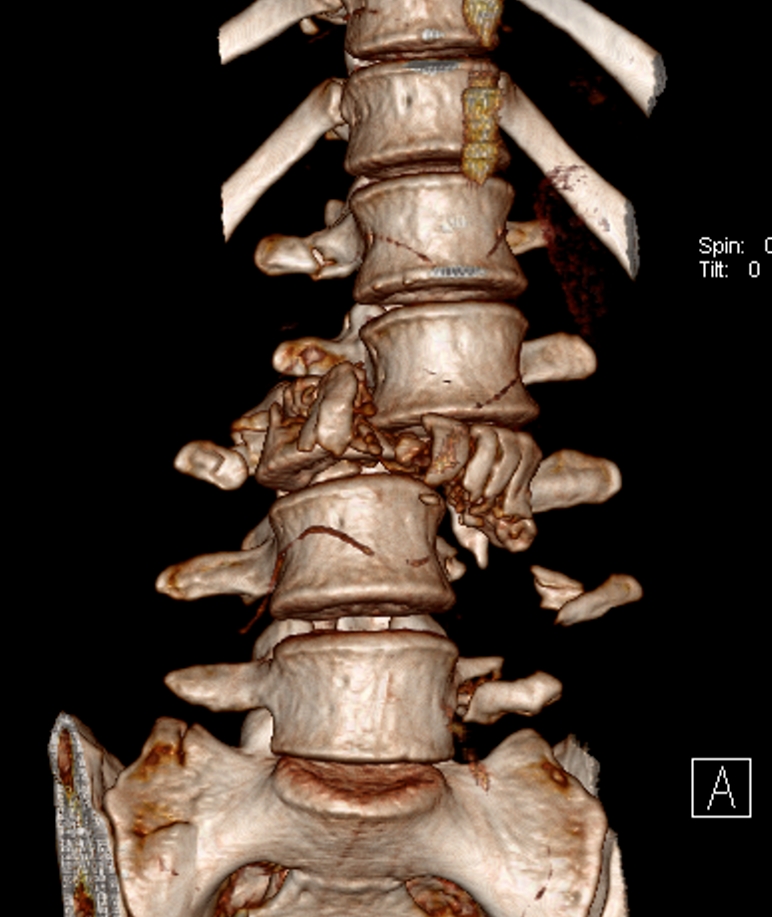
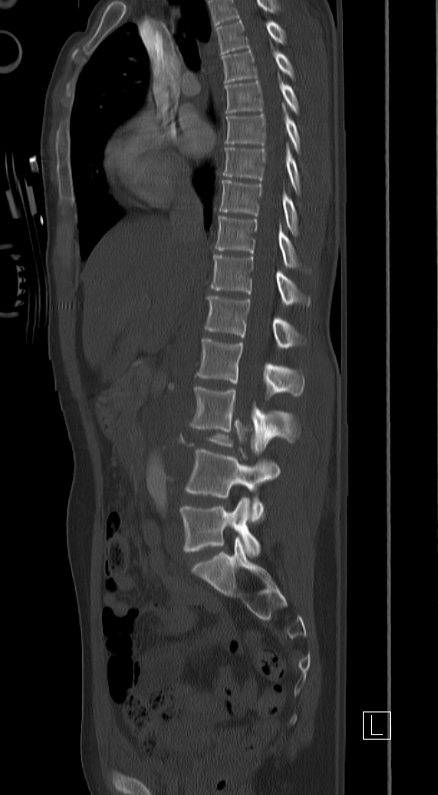
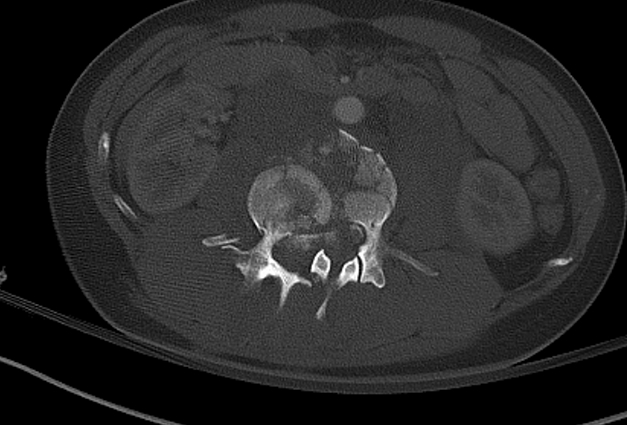
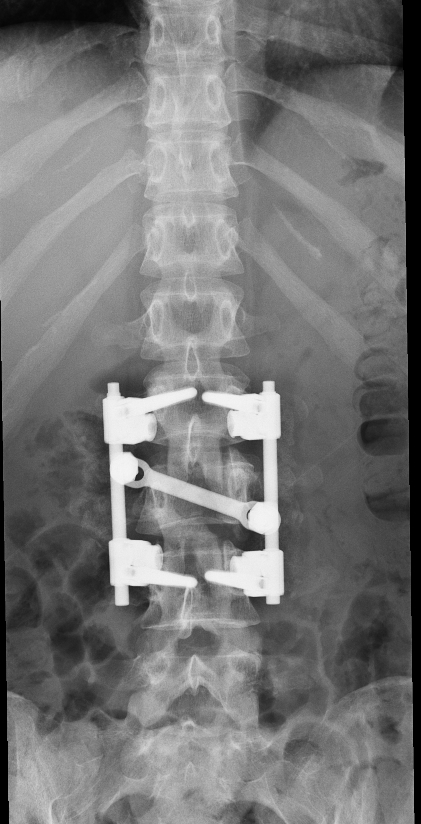
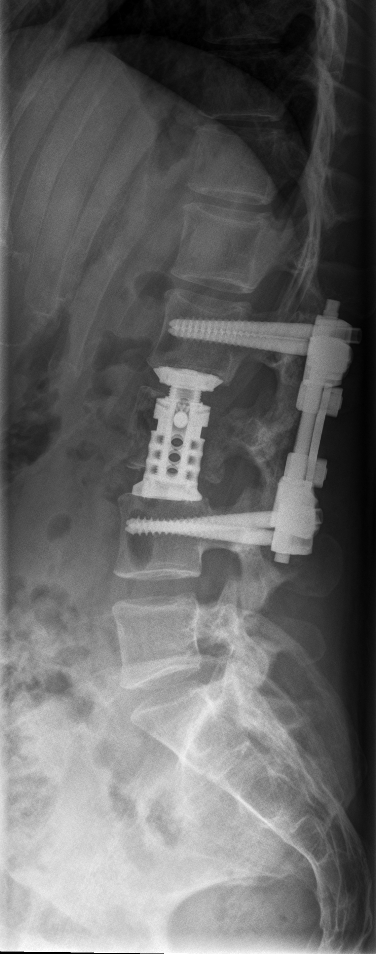
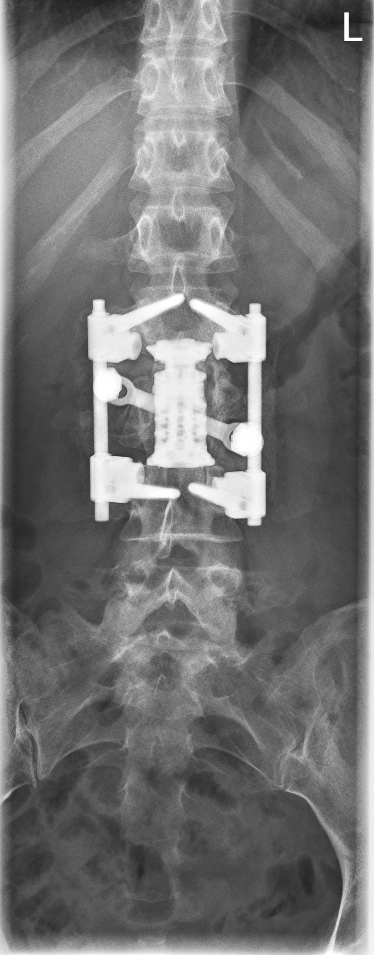
An example of surgical treatment of lumbar spine injuries. A patient with a severe, fragmentary fracture of the 3rd lumbar vertebra struck by a car. Surgical therapy in two periods, primarily posterior correction and fixation with a transpedicular internal fixator with removal of the oppression of nerve structures, followed by anterior replacement of the L3 body with an expandable implant after a few days.




- Teaching
- Publications
- Books
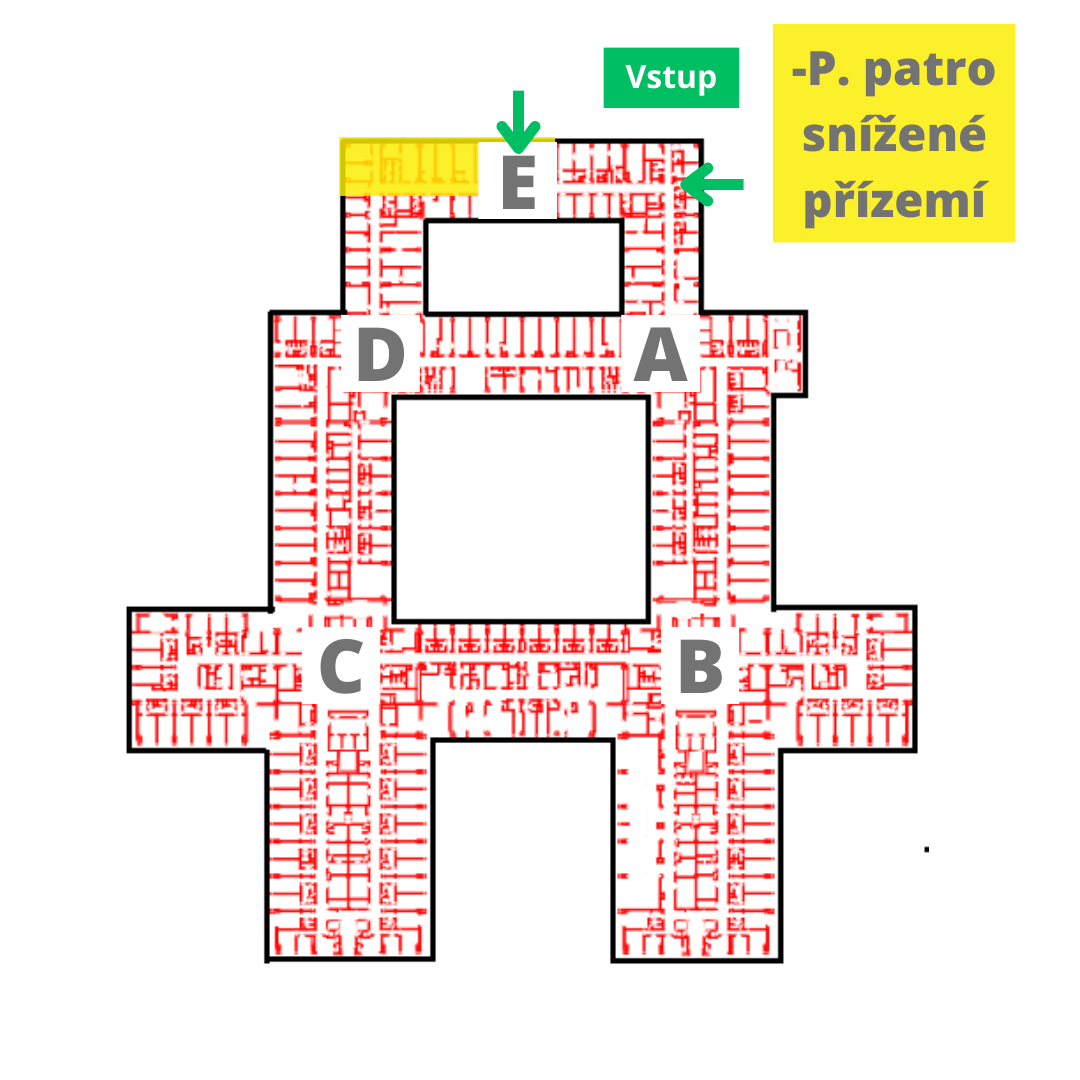
| From November 9, 11, the spondylosurgery outpatient clinic, including the Conservative Therapy Center, has been moved to the lower ground floor – P floor, node E. |
Dear Madam, dear Sir,
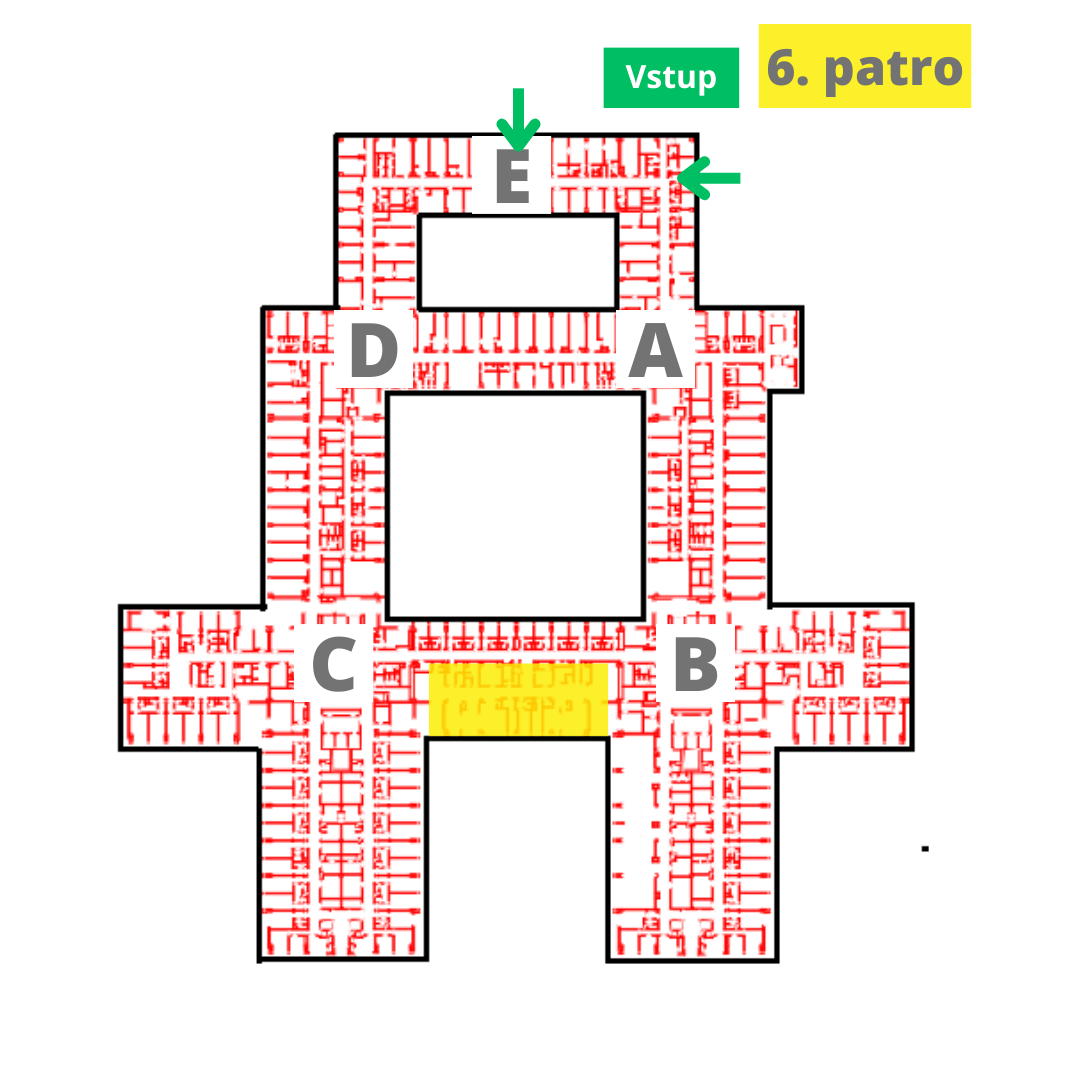
you will arrive at our clinic on the day of admission, 6th floor / node B, FN Motol, adult part, best between 9-10 o'clock in the morning to the admissions office. It is located just after entering the department on the left. Here, the administrative staff of our secretariat will handle the most important formalities with you (verification of identity and personal data, health insurance and their entry into the hospital system). Subsequently, you will be admitted by a pre-designated doctor at the ward - they will take a medical history, perform a clinical examination focusing on the examination of the spine, check and prepare the results of imaging examinations, e.g. fills in the missing. The doctor will further instruct you about the nature of the disease and the possibilities of therapy with a focus on the method and course of the operation. They will also explain the complications that may occur during surgery and hospitalization. If you agree with the proposed procedure, you will sign the necessary informed consents (with hospitalization, surgery and administration of blood derivatives). Furthermore, you will be received by a nurse / brother, who will then place you in a predetermined bed. Standard rooms are triple, equipped with private toilet and shower, LCD TV. They are in the standard department of the clinic 2 single superior rooms, in which we provide above-standard accommodation, the room price is 1500 CZK/night. More at the FN Motol stands.


On the day of your admission, there may be a delay between the admission itself and the bedtime, which is due to the necessary administration associated with admitting new and dismissing existing patients. In the afternoon, the anesthesiologist checks it and prepares it before general anesthesia the following day. Patient order the primary department or his deputy always determines the operation for the operation. The order may vary, with preference given to patients with acute spinal disease who have been admitted during the service. Therefore, your planned operation may be postponed or even canceled. We ask for leniency and tolerance with patients who have entered our ward in an acute condition.
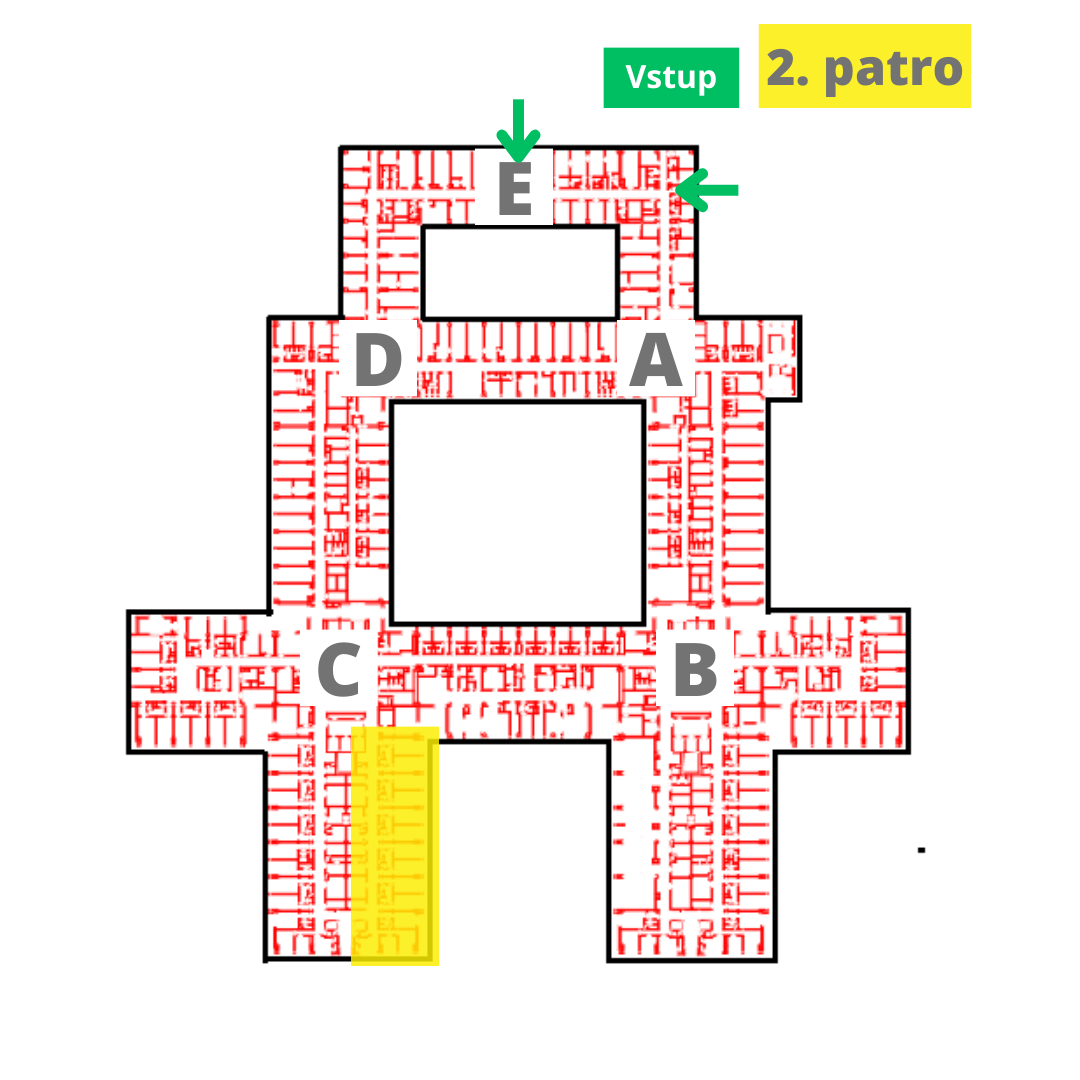
Immediately after surgery you will be saved on intensive care unit (node C, 2nd floor), where you will be intensively monitored according to the severity of the operation and your clinical condition. You will also be given effective analgesic therapy, chronic medicines, medicines to prevent deep vein thrombosis and other symptomatic therapies. The length of hospitalization in the intensive care bed is usually 1-3 days with an uncomplicated postoperative course. On the 1st postoperative day, if your condition allows, we will perform a follow-up imaging examination. 2. postoperatively, you will be instructed by the physiotherapist about the movement regime and gradually verticalized with his assistance.

After stabilization of your condition, a translation on a standard bed follows. The practice of verticalization and mobilization, self-service, continues. We will gradually reduce analgesic therapy so that you can be released home without its significant support. The average length of hospitalization in our ward is six days.
If you have any during hospitalization any questions or doubts, don't be afraid to ask your doctor during visits that take place every morning.
Rehabilitation after thoracic and lumbar spine surgery
Dear patient, you have undergone spine surgery at the Department of Spondylosurgery, University Hospital in Motol. We would like to provide you with recommendations on how to behave in the home environment after thoracic or lumbar spine surgery. You should be aware that your spine is still ill and that only the cause of the pain, which is the result of more wear and tear on the spine as a whole, has been removed by surgery. Therefore, it is necessary to recommend how you should treat the diseased spine. These recommendations are also indicated for patients after thoracic or lumbar spine surgery after an injury without a neurological deficit.
Dear patient,
you have undergone spine surgery at the Department of Spondylosurgery, University Hospital in Motol. We would like to provide you with recommendations on how to behave in the home environment after thoracic or lumbar spine surgery.
You should be aware that your spine is still ill and that only the cause of the pain, which is the result of more wear and tear on the spine as a whole, has been removed by surgery. Therefore, it is necessary to recommend how you should treat the diseased spine.
These recommendations are also indicated for patients after thoracic or lumbar spine surgery after an injury without a neurological deficit.
1. On the way home, the nurses will provide you with an ambulance according to the doctor's indication, the transport will take place lying down.
Upon arrival at home, if possible, we recommend staying mostly in bed. The ambulance journey is a sufficient burden for this day.
2. In a home environment, it is advisable to sleep on a flat, raised bed so that you can get up as best you can.
3. Initially, it is advisable to climb the stairs only when accompanied by another person, as a situation may arise in which someone will need to provide you with support.
4. You can put the crutches down briefly while sitting in the toilet. You can start sitting only after the first check-up with a spondylosurgeon, which is usually six weeks after the operation. However, a longer session and complete postponement of the crutches is indicated by the doctor up to three months after the operation.
If you already get permission to sit down, you should start carefully, only for a short time, for example to eat. You should always sit with your back straight. However, you must avoid sitting in a car or a chair for a long time.
Depending on your general health, you can prolong walking outdoors.
5. It is good to practice learned exercises several times a day. Temporarily skip painful exercises.
6. You should avoid movements that are related to the surroundings of the operation site, such as bows, bends, tilts, and rotations. These movements may begin to train slowly up to three months after surgery.
7. We recommend not doing hard physical work, not lifting heavy objects. If necessary, you can get up from a squat and a straight back. Sudden uncoordinated movements, such as slipping, should be avoided. Be careful when walking on uneven terrain.
8. You can shower around the surgical wound after removing the stitches, then it is advisable to dry the wounds with touches and finally lubricate them with a greasy cream.
Bathing in hot water after surgery is not recommended.
9. Rehabilitation is usually indicated at the FNM Department of Spondylosurgery up to three months after surgery.
10. Driving a car while sitting is contraindicated, that is, it is prohibited.
11. Sexual activity is possible if it is not accompanied by pain from the operating field. It is therefore necessary to choose a position in which the spine is relieved, also for a period of three months.
12. We do not recommend sports until six weeks after the operation, the only thing that can be recommended is passive exercise. This is an exercise that allows you to maintain full range of motion in the joints and flexibility of muscles and tendons.
13. After three months, you can slowly start sports such as swimming or cycling.
14. You are entitled to spa treatment within 1 year after the operation. It is advisable to undergo spa treatment about half a year after the operation.
Scar care
The goal of scar care is to heal well and to ensure that the scar moves against the subcutaneous tissue and other structures. It occurs when there are no more scabs on the scar and the skin is completely healed. Let the scar heal, do not tear the scabs around it. Shower the scar for you with a pleasant stream of lukewarm water, but in the first weeks do not soap it, just rinse with water. Keep the scar clean, dry it carefully after bathing and apply a greasy unscented cream to it - this will ensure its suppleness. Apply a so-called pressure massage to the scar (see below). The scar must not be red, hot, purulent and must not bleed.
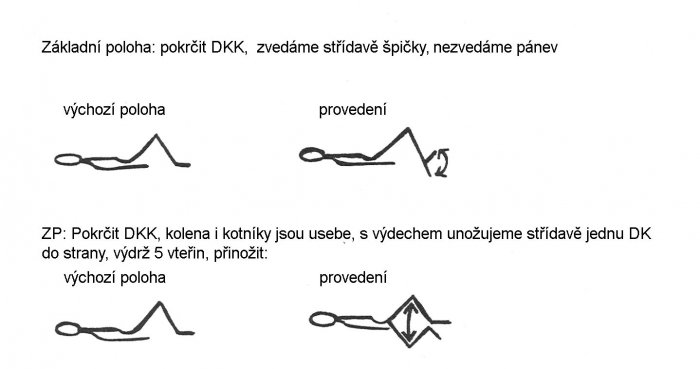
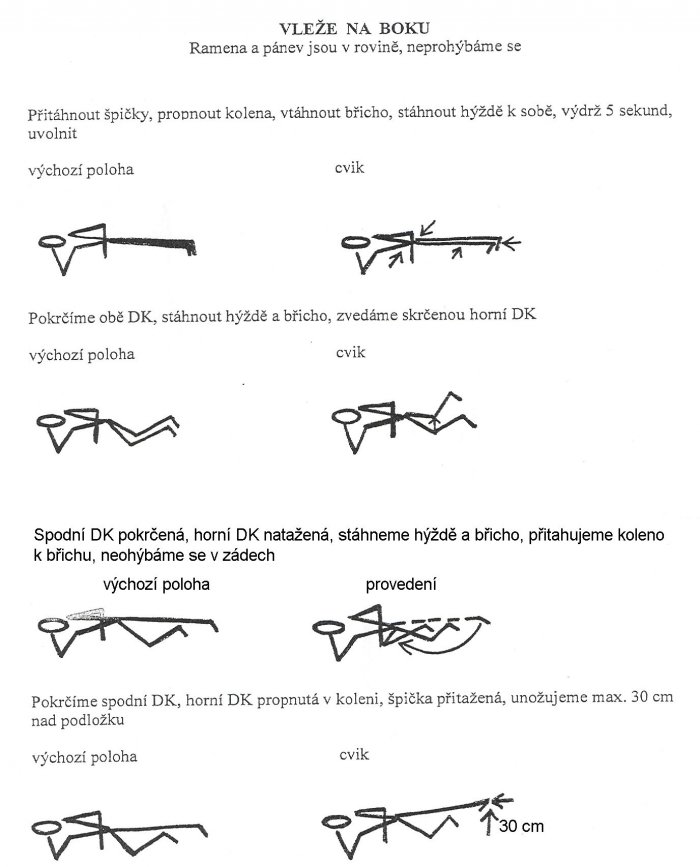
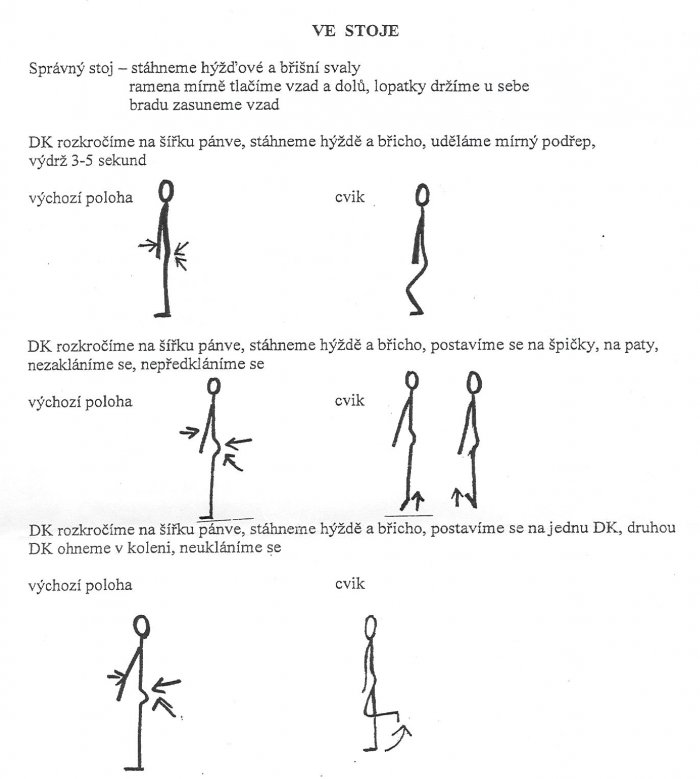
Exercise unit after lumbar spine surgery
We follow these principles during the exercise:
- We practice slowly
- We perform exercises slowly with a pull, not a swing
- Exercises must not cause pain, if so, we will skip these exercises
- We take 10-second breaks between each exercise
- We breathe regularly during exercise, we do not hold our breath
- We repeat each exercise 5 times, gradually increasing the number of repetitions
- We exercise regularly several times a day
Explanatory notes:
HK ........ one upper limb DK ....... lower limb
HKK ..... both upper limbs HD .... both lower limbs
Walking up the stairs with armpits:
to the stairs: from the stairs
1. First DK 1. Both crutches at once
2. Second DK 2. First DK
3. Both crutches at once 3. Second DK
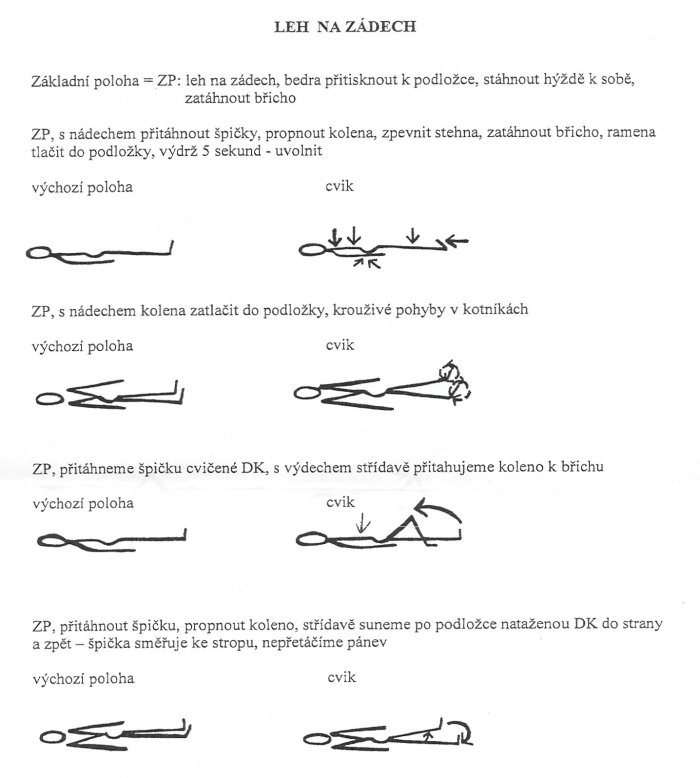
ZP: crease HD, then with a breath pull the buttocks and abdomen, endurance 5 seconds, relax:

Rehabilitation after cervical spine surgery
Rehabilitation after cervical spine surgery Dear patient, You have undergone cervical spine surgery at the Department of Spondylosurgery, University Hospital in Motol. We would like to provide you with recommendations on how to behave in the home environment after cervical spine surgery. 1. On receipt, you received a fixed Philadelphia neck collar, which is fully paid for by the insurance company. However, the insurance company only pays for the collar per calendar year, so it is very important that you treat the collar with care, as you will have to wear it for six weeks according to your doctor's prescription. The collar should be washed daily with lukewarm water, aggressive detergent should not be used. It is best to wash it with lukewarm soapy water, then rinse with clean water and dry properly. Please do not modify the collar to your liking, as only the standard collar performs its function.
you have completed cervical spine surgery at the Department of Spondylosurgery, University Hospital in Motol. We would like to provide you with recommendations on how to behave in the home environment after cervical spine surgery.
1. Upon receipt, you received a tight Philadelphia neck collar, which is fully paid for by the insurance company. However, the insurance company only pays for the collar per calendar year, so it is very important that you treat the collar with care, as you will have to wear it for six weeks according to your doctor's prescription.
The collar should be washed daily with lukewarm water, aggressive detergent should not be used. It is best to wash it with lukewarm soapy water, then rinse with clean water
and dry properly.
Please do not modify the collar to your liking, as only the standard collar performs its function.
2. The correctly fitted collar must not strangle or be loose. The velcro you fasten it with should be placed on top of each other.
3. When removing the collar, eg during hygiene, avoid rotation of the head and forward bends.
4. You can lie in bed without a collar, with your head from the shoulders underlain by a soft, low-filled pillow. The cervical spine must be level. If you have a restless sleep and are aware of the constant rotation on the bed, you better sleep with your neck collar.
5. The sutures on the neck after anterior access surgery are sewn with absorbable material, so you don't have to come out.
6. The surgical wound on the neck after surgery from the posterior approach is sutured with non-absorbable sutures and therefore must be removed over time. This is usually done (according to the doctor's office) 14 days after the operation.
7. The surgical wound after graft removal is sutured with non-absorbable sutures, so it is necessary to remove them as well. This happens (according to the doctor's office) 14 days after the operation.
8. After 14 days, once the surgical wounds have healed, it is recommended to lubricate them with cream or body lotion to make the scar soft. The scar completely fades
even several months, depending on the ability of the body to regenerate.
Do not soak or bathe surgical wounds. In case of redness, pain, feeling of heat or twitching in the surgical wound, it is necessary to arrange a check-up at the spondylosurgery clinic.
9. Carry out all household chores with the neck collar, loads in the hands may be carried up to a total weight of seven kilograms.
10. Sports is not recommended six weeks after surgery, the only thing that can be recommended is passive exercise. This is an exercise that allows you to maintain full range of motion in the joints and flexibility of muscles and tendons.
11. You do not have to give up sex life, it only depends on you and your partner, or on the choice of a gentle sexual position.
12. You can come to the outpatient clinic of the spondylosurgery department as a co-driver by car or public transport, the ambulance is no longer indicated.
Scar care
The goal of scar care is to heal well and to ensure that the scar moves against the subcutaneous tissue and other structures. It occurs when there are no more scabs on the scar and the skin is completely healed. Let the scar heal, do not tear the scabs around it. Shower the scar for you with a pleasant stream of lukewarm water, but in the first weeks do not soap it, just rinse with water. Keep the scar clean, dry it carefully after bathing and apply a greasy unscented cream to it - this will ensure its suppleness. Apply a so-called pressure massage to the scar (see below). The scar must not be red, hot, purulent and must not bleed.
Pressure massage
Place the thumb of one hand on the lower edge of the scar and lightly press it against the scar with tolerable intensity. After a few seconds, release your thumb, which increases the blood supply to the scar at the site of compression. Follow the same procedure along the entire length of the scar.
Grasp the scar with the so-called fork (between the outstretched index finger and the middle finger) - this will create an eyelash, which you can easily move to the right and left with that "fork". The displacement of the scar is not large at all. Then loosen everything and proceed in the same way along the entire length of the scar.
We wish you a speedy recovery.
The staff of the spondylosurgery clinic
Baggage to the hospital
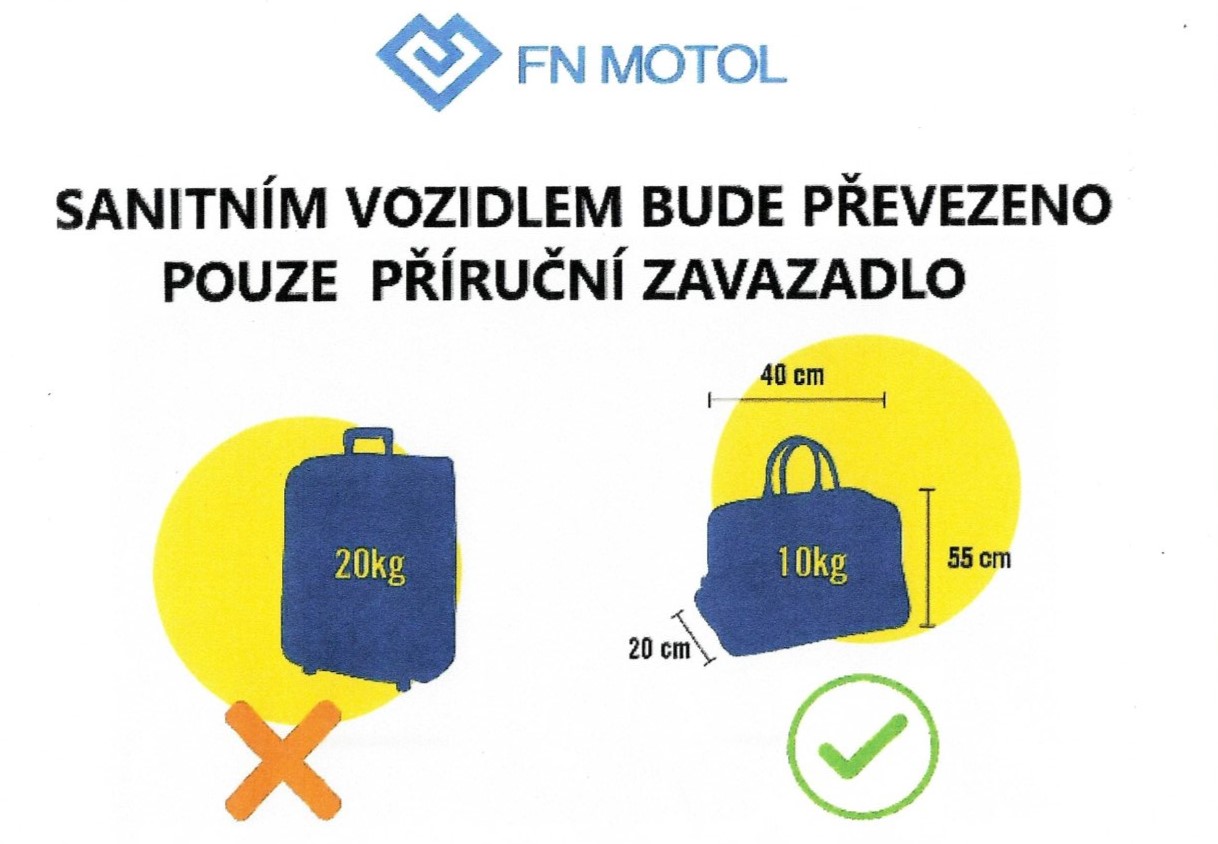
PATIENT AFTER HEAD AND LUMBUM
- GETTING UP FROM THE BED
- IN THE OPPOSITE ORDER OF PHOTOS, THE LAYING TO THE BED IS SHOWED
1.

POSITION ON THE ABDOMEN
- the patient turns onto the abdomen
- lies on the edge of the bed
- both upper limbs are at the head
2.a

LOWERING THE LIMBS FROM THE BED TO THE GROUND
- The first lowered limb is the limb closer to the edge of the bed
- the foot touches the ground
- the knee is slightly bent
- the patient's weight begins to be transferred to the lowered lower limb and both elbows
2.b

LOWERING THE LIMBS FROM THE BED TO THE GROUND
- the knee is slightly bent
- The patient's weight is transferred to the lowered lower limb and both elbows, the patient lifts the upper half of the body
- the spine must not be bent at the shoulders!
2.c
LOWERING THE LIMBS FROM THE BED TO THE GROUND
- the patient's weight is constantly transferred to the lowered lower limb
- the weight from the elbows is gradually transferred to both palms
- the spine must not be bent at the shoulders!
3.

LOWERING THE SECOND LOWER LIMBS ON THE GROUND
- the second lower limb is gradually lowered to the ground
- both knees are slightly bent, the patient is squatting slightly
- the patient's weight is transferred to both lower limbs
- palms lightly touching the bed
- the spine is in one plane
(without excavation of the spine and its rotation)!
4.

STAND IN THE BED
- straight knees
- flattened spine
- then the patient puts on his crutches
All the steps of getting up and laying in bed follow each other smoothly.
With the promise of the possibility of establishing an independent specialized spondylosurgical department, Dr. In November 2001, Štulík moved from the orthopedic-trauma clinic of the FNKV to the 1st orthopedic clinic of the Motol University Hospital. Here he began to devote himself entirely to spine surgery. Within the standard orthopedic department, three rooms were set aside and one operating day for elective surgery. Traumas were treated separately in the trauma operating room.
Due to the growing number of patients and surgical procedures, it was possible to establish a completely independent department within a few months. On September 1, 2002, the spondylosurgery department of the Motol University Hospital was opened. Organizationally as half of one unit together with the department of neurosurgery for adults, which has been missing in Motol so far. The two separate primates thus had a common secondary medical staff. Operating room for elective operations available on Tuesdays, Thursdays and every even Friday, then gradually every Friday. Subsequently, there was a complete separation of the hall and soon the division of the department, when the neurosurgery moved to the newly allocated premises.
The beginning of the establishment of an independent department dates back to the establishment of the Spondylosurgery Center of the Motol University Hospital, which was established from representatives of individual specializations to determine algorithms for care of patients with spine and spinal cord diseases at the Motol University Hospital and the treatment was rational and as effective as possible.
Since 2007, our workplace has been part of III in terms of teaching. surgical clinics of the 1st Medical Faculty of Charles University and the University Hospital Motol. We are mainly engaged in teaching 5th and 6th year students of the 1st Faculty of Medicine, Charles University and postgraduate education of domestic and foreign doctors in the field of spondylosurgery. We also work closely with the 1st Department of Surgery, 1st Faculty of Medicine, Charles University and General Hospital, 1st Department of Orthopedics, 1st Faculty of Medicine, Charles University and Motol University Hospital, Department of Orthopedics, 1st Faculty of Medicine, Charles University and General Hospital, Department of Orthopedics, XNUMXst Faculty of Medicine, Charles University and Central Hospital.
During its operation, the department ranked first in the classification of domestic workplaces according to the CSCH database of spondylosurgical procedures. The department concentrates up to 25% of all spinal injuries in the Czech Republic, and is also focused on the treatment of primary spinal tumors in children and adults, spinal deformities in children and adults, and craniocervical junction surgery. In the field of extensive tumor resections, the department developed, tested and published new surgical techniques generally accepted in our country and abroad.
Since its establishment in 2002, the Motol Department of Spondylosurgery has published a total of 60 papers in domestic and foreign journals (22 publications in journals with IF, total IF value 29,874, average IF value 1,358). A total of 4 works were awarded the Zahradníček Prize for the best publication of Acta Chir magazine. Orthop. Traumatol. Guild. In 2010, a book was published Cervical spine injuries, which was published in 2012 in the English version as Cervical Spine Trauma. The book won the Chlumský ČSOT Award for the best publication in 2013 and was also awarded by the Rector of Charles University.
On January 1, 2016, the Department of Spondylosurgery of the 1st Medical Faculty of Charles University and the Motol University Hospital was established, as the first of its kind in the Czech Republic, following the example of foreign university centers. This act means a significant contribution to the development of spondylosurgery in the Czech Republic, for its undergraduate and especially postgraduate teaching.
Department






























































Ambulance

















Operating room


















Contact
General contacts
- Secretariat: Zachová Renata, tel .: 224 432 581
Email: renata.zachova@fnmotol.cz - Standard department, tel .: 224 432 573
- ICU, tel .: 224 432 590
- Ambulance, patient ordering, tel .: 224 432 592
- Center for conservative therapy in spondylosurgery, MUDr. Eva Vašková, phone: 224 432 575, 224 432 576
- Admissions office: phone: 224 432 571, fax: 224 432 584
Naděžda Popelková, e-mail: nadezda.popelkova@fnmotol.cz
Václava Masopustová, e-mail: vaclava.masopustova@fnmotol.cz
Tereza Pittnerová, e-mail: tereza.pittnerova@fnmotol.cz
Where to find us?
 |  |  |
|
|
|