Basic information
 Dear friends, colleagues, co-workers and sponsors, pediatric patients and their parents!
Dear friends, colleagues, co-workers and sponsors, pediatric patients and their parents!
The Department of Pediatrics of the 2nd Faculty of Medicine of Charles University and the University Hospital in Motol was established in 2004 by merging the work teams of the former I. children's clinic and a significant part of the former II. children's clinic. It is a continuation of their mission - to provide highly specialized and erudite care to children from all over the Czech Republic, whose doctors or parents have requested it. The team of the Pediatric Clinic creates a natural professional background, the "ultimum refugium", for all Czech and Moravian pediatricians, whether they work in children's clinics of teaching hospitals, district children's wards or work as general practitioners for children and adolescents. We are ready to help you and your patients whenever you deem it necessary.
You also meet the staff of the Pediatric Clinic in undergraduate and postgraduate education in pediatrics and its subspecializations, in organizational activities in the care of sick children at the national level and in clinical research and development of biomedical knowledge for the benefit of pediatric patients.
In almost all areas of pediatrics and adolescent medicine, the Pediatric Clinic has highly qualified specialists who provide top diagnostics and therapy - in pediatric nephrology, dialysis and elimination methods, pediatric pneumology, allergology and care for children with cystic fibrosis, pediatric endocrinology and diabetology. , in pediatric gastroenterology and in the care of children with autoimmune diseases. In cooperation with partner workplaces of the Motol University Hospital, we also provide cardiological, immunological and hematological care.
The credo of the Pediatric Clinic team is "partnership for the benefit of pediatric patients". We are here for you and your patients. Our strength lies in the team experience, in the quality equipment and in the cooperation of the pediatric think tank of the Motol hospital. We strive for straightforward, fast and effective diagnosis and therapy with maximum care for our common pediatric patients.
Our work would be more difficult without sponsors, who make a significant contribution to the renewal and expansion of the clinic's equipment, our "instruments", but also to a friendly and aesthetic environment for our patients. Many thanks to all our sponsors, the clinic team and our patients.
Thanks also go to all Czech and Moravian pediatricians in primary care and inpatient facilities. We highly value their daily endless efforts. It is thanks to them and their work that the sick children who need it most come to us. We thank them for recommending and sending these patients to us. I am sure that it is through our joint efforts that we achieve the maximum possible for the well-being of sick children.
Prof. MUDr. Jan Lebl, CSc., On behalf of the team of doctors and nurses of the Pediatric Clinic
The head
Prof. MUDr. Zdenek Sumnik, Ph.D.
Primary
doc. MD Štěpánka Průhová, Ph.D.
224 432 003
pediatrie@fnmotol.cz
Other contacts
Medical Secretariat
224 432 002
jana.saskova@fnmotol.cz
224 432 004
lenka.viktorinova@fnmotol.cz
School secretariat
224 432 001
klara.borecka@fnmotol.cz
Contact with health insurance companies
224 432 007
jitka.doubravova@fnmotol.cz
Center for comprehensive care for children with developmental disorders and their families
Viz Center for comprehensive care for children with developmental disorders and their families
Center for Diagnosis and Treatment of Ciliary Epithelial Disorders (Primary Ciliary Dyskinesia)
The Center for Ciliary Epithelial Disorders at the University Hospital in Motol is the main workplace in the Czech Republic providing diagnosis and treatment for patients with this congenital disorder.
The Motol Center has been dealing with this topic for many years, in the last few years the center's equipment has been significantly improved and diagnostic methods and treatment procedures have been introduced in the form usual in most developed countries. It was also possible to significantly increase the detection of patients with this disorder, which allows for the timely introduction of medical care and thus improve the prognosis. Primary ciliary dyskinesia (PCD) is a rare disease, its incidence in our country is expected to be similar to that of cystic fibrosis, ie about 600 individuals. However, we still lack to detect about 500 patients with this number. They may be hiding under other diagnoses and thus do not receive proper comprehensive care. Their disease then unnecessarily causes them a number of significant problems and unnecessarily damages the lung tissue. We are therefore trying to raise awareness of this disease both among the general public and among health professionals.
Detailed information about our center and the disease can be found on the website www.rasinky.cz
Our workplace is a full member of the European Reference Network (ERN-LUNG). ERN-LUNG is dedicated to providing and supporting the care of patients suffering from rare respiratory diseases on a global scale. It is committed to the prevention, diagnosis and treatment of rare respiratory diseases through very high levels of patient care, education and research.
We are also part of the Clinical Trial Network (CTN), which will give PCD patients access to experimental drugs, the development of which gives much hope. In the case of PCD, drugs have not yet been developed to address the underlying cause of the disease. However, clinical trials do not forget the treatment of complications associated with the underlying disease, which include clinical trials of antibiotics and anti-inflammatory drugs to treat lung infections and inflammation.
Center for highly specialized care for rare liver diseases
Our center is part of the European Reference Network for Rare Liver Diseases (ERN RARE-LIVER). These are highly specialized centers, which were created in order to improve the quality of care for patients with rare diseases and the possibility of mutual international scientific cooperation.
The Motol Center is part of a consortium with the Department of Hepatogastroenterology of the Prague Institute of Clinical and Experimental Medicine (IKEM, www.ikem.cz), which is the largest center for liver disease in the Czech Republic and specializes in the care of patients included in the liver transplant program. The Department of Pediatric Gastroenterology and Hepatology at FNM provides a full range of diagnostic and therapeutic methods and procedures in the field of diseases of the digestive tract and liver. It is an accredited workplace in the field and the largest children's hepatology center in the Czech Republic. It provides care for patients with acute and chronic liver disease, especially patients with biliary atresia, genetic cholestatic disease, including Allagill's syndrome, as well as patients with autoimmune hepatitis, primary sclerosing cholangitis or Wilson's disease.
Center representatives:
FN Motol:
MUDr. Radana Kotalová, CSc., Chief Coordinator of the Center
MUDr. Katarína Mitrová, Ph.D., Deputy Chief Coordinator
MD Marianna Durilová, Ph.D.
MD Eva Vlčková
IKEM:
doc. MUDr. Jan Šperl, CSc., Chief Coordinator of the Center
prof. MUDr. Mgr. Milan Jirsa, CSc., Deputy Chief Coordinator
https://www.ikem.cz/cs/transplantcentrum/klinika-hepatogastroenterologie/a-33/
Dear friends, colleagues, co-workers and sponsors, pediatric patients and their parents!
The Department of Pediatrics of the 2nd Faculty of Medicine of Charles University and the University Hospital in Motol was established in 2004 by merging the work teams of the former I. children's clinic and a significant part of the former II. children's clinic. It is a continuation of their mission - to provide highly specialized and erudite care to children from all over the Czech Republic, whose doctors or parents have requested it. The team of the Pediatric Clinic creates a natural professional background, the "ultimum refugium", for all Czech and Moravian pediatricians, whether they work in children's clinics of teaching hospitals, district children's wards or work as general practitioners for children and adolescents. We are ready to help you and your patients whenever you deem it necessary.
You also meet the staff of the Pediatric Clinic in undergraduate and postgraduate education in pediatrics and its subspecializations, in organizational activities in the care of sick children at the national level and in clinical research and development of biomedical knowledge for the benefit of pediatric patients.
In almost all areas of pediatrics and adolescent medicine, the Pediatric Clinic has highly qualified specialists who provide top diagnostics and therapy - in pediatric nephrology, dialysis and elimination methods, pediatric pneumology and care for children with cystic fibrosis, pediatric endocrinology and diabetology, in pediatric gastroenterology and in the care of children with autoimmune diseases. In cooperation with partner workplaces of the Motol University Hospital, we also provide cardiological, immunological and hematological care.
The credo of the Pediatric Clinic team is "partnership for the benefit of pediatric patients". We are here for you and your patients. Our strength lies in the team experience, in the quality equipment and in the cooperation of the pediatric think tank of the Motol hospital. We strive for straightforward, fast and effective diagnosis and therapy with maximum care for our common pediatric patients.
Our work would be more difficult without sponsors, who make a significant contribution to the renewal and expansion of the clinic's equipment, our "instruments", but also to a friendly and aesthetic environment for our patients. Many thanks to all our sponsors, the clinic team and our patients.
Thanks also go to all Czech and Moravian pediatricians in primary care and inpatient facilities. We highly value their daily endless efforts. It is thanks to them and their work that the sick children who need it most come to us. We thank them for recommending and sending these patients to us. I am sure that it is through our joint efforts that we achieve the maximum possible for the well-being of sick children.
Prof. MD Jan Lebl, CSc.,
on behalf of the team of doctors and nurses of the Pediatric Clinic









Doctors
Knowledge:
head - Prof. MUDr. Zdenek Sumnik, Ph.D.
Chief Medical Officer – primary doc. MD Štěpánka Průhová, Ph.D.
head nurse - Mgr. Jana Boháčová
Working groups, inpatient departments, outpatient clinics and laboratories of the Pediatric Clinic:
- pediatric nephrology working group with inpatient department and outpatient clinic - head doc. MUDr. Jakub Zieg, Ph.D.
- inpatient department of pediatric nephrology - head doc. MUDr. Jakub Zieg, Ph.D., station nurse Mgr. Petra Janásová
- Department of Dialysis and Elimination Methods - Head MUDr. Naděžda Šimánková, station nurse Eva Vlachová
- pediatric nephrology clinic - head MUDr. Naděžda Šimánková
- working group of pediatric pneumology, allergology, cystic fibrosis and cardiology and the inpatient ward, outpatient clinics, endoscopic examination rooms and laboratories - head prof. MUDr. Petr Pohunek, CSc.
- inpatient department of children's respiratory diseases - head MUDr. Tereza Doušová, station nurse Hana Benešová
- cystic fibrosis center - head of the clinical part MUDr. Veronika Skalická
- lung functional diagnostics laboratory - head prof. MUDr. Petr Pohunek, CSc.
- cardiology outpatient clinic and ECG laboratory - MUDr. Veronika Stará
- working group of pediatric endocrinology, diabetology and autoimmune diseases with inpatient department, outpatient clinics and laboratories - head prof. MUDr. Jan Lebl, CSc. and prof. MUDr. Zdenek Sumnik, PhD.
- inpatient department of pediatric endocrinology and diabetology - head prof. MUDr. Zdeněk Šumník, PhD., Station nurse Radomíra Kučerová
- outpatient department of pediatric endocrinology, diabetology and anthropology - head MUDr. Stanislava Kolouskova, CSc.
- molecular genetics laboratory - head prof. MUDr. Ondrej Cinek, PhD.
- working group of pediatric gastroenterology, hepatology and nutrition with inpatient department, endoscopic examination rooms, ambulances and laboratories - head doc. Jiří Bronský, MD, Ph.D., station nurse Jitka Doubravová
- inpatient department of infant medicine with an ambulance - head doc. MUDr. Květa Bláhová, CSc., Station nurse Jiřina Mašková
- intensive care unit of the Pediatric Clinic inpatient department - chief physician doc. MUDr. Filip Fencl, Ph.D., station nurse Ivana Hindráková
Information for patients
The Pediatric Clinic of the Motol University Hospital is a specialized pediatric institution which, in addition to medical and preventive care for young patients, also deals with teaching and research. Due to the high professional level of its physicians, the clinic ranks among the so-called "supraconsiliary workplaces" - it normally acts as an advisory body for other workplaces and physicians who may need advice or professional guidance in some very complex and rare care situations for pediatric patients.
The clinic has 90 beds, of which 30 are intensive care beds. They are divided into 5 departments and an outpatient dialysis-transplant unit for patients with chronic kidney disease. The clinic also includes a gastroenterology laboratory and a laboratory for molecular genetics.
You can find contacts for individual workplaces in the section Contact , more about individual working groups can be found in the tab Working groups.
Turner syndrome
Authors:
Prof. MD Jan Lebl, CSc.
Doc. MUDr. Jirina Zapletalova, Ph.D.
Download full text: Turner syndrome [doc; 167,0 kB]
Introduction
This text deals with Turner syndrome, its causes and manifestations, and its treatment. It was created to provide information and instruction to all who are directly affected by Turner Syndrome - parents of girls with Turner Syndrome, older girls and women themselves, but also their doctors, who do not encounter Turner Syndrome often.
The text summarizes the findings on all known aspects of Turner syndrome. Girls and women who understand "their" Turner syndrome are known to be much more balanced and happier than those for whom their medical condition remains an incomprehensible secret. It is useful to familiarize Turner Syndrome with the wider family, teachers who have a girl with Turner Syndrome in their class and later, in upper school classes, as well as classmates and girlfriends of girls. The new information will also help them understand a certain difference in their good friend with Turner syndrome.
This text is intended for all of them.
1. How does Turner syndrome arise?
The human body is made up of many billions of individual cells. Every cell in our body has an assembly of 46 chromosomes in its cell nucleus. And each of these chromosomes carries a number of genes, carriers of genetic information. Genes are written on chromosomes in the form of a complex chemical compound called deoxyribonucleic acid (DNA). It is the genes that largely determine what a person will be. If he is big or small, blonde or dark-haired, brown-eyed or blue-eyed, what will be the features of his face, whether he will have musical or motor talent, and how developed will his spatial imagination, necessary for school success in mathematics or descriptive geometry. We could go on for a long time in this list of gene-borne traits. The genes stored in the chromosomes thus decisively determine both the physical characteristics of the human individual and his mental abilities.
At each cell division, the same set of 46 chromosomes is transferred to each emerging cell. Thus, a person has exactly the same set of chromosomes in each cell of his body that accompany him throughout his life.
44 of the 46 chromosomes are called autosomes. Their appearance is the same for women and men. The other two chromosomes are called heterochromosomes, or sex chromosomes. They decide whether the emerging little man will be a boy or a girl and grow up once into an adult man or an adult woman. Women have two female sex chromosomes, the "X" chromosomes. Therefore, their chromosome assembly (or karyotype) indicates 46, XX. In this formula, the number "46" denotes the total number of chromosomes and "XX" two female sex chromosomes X. Men, on the other hand, each have their own sex chromosome - one male "Y" and one female "X". Their set of chromosomes (karyotype) is described as 46, XY.
The future new man acquires his chromosomes just half from his mother and half from his father. The mother's egg carries 23 chromosomes in its nucleus, and one of them is the sex chromosome "X". Paternal sperm also carries 23 chromosomes. There is also one sex chromosome, in half of the cases the "X" chromosome, in the other half of the cases the "Y" chromosome. As a result, half of the girls and half of the boys are born. When a mother's egg is fertilized by paternal sperm, the two sets of chromosomes merge to form a definitive set of 46 chromosomes (23 pairs), which the new man obtains from his parents and which he will carry throughout his life. At this point, the gender of the future human individual will be decided. We see that the sex chromosome, brought by sperm, is decisive. An egg fertilized by sperm with the "X" chromosome turns into a girl, while fertilizing sperm with a "Y" chromosome results in a boy.
If an egg or sperm yields one chromosome less, or if one of the chromosomes is lost when they merge with each other, a set of 45 chromosomes is formed. If one sex chromosome is missing and only one "X" chromosome remains, the new human will have karyotype 45, X. And this is a typical karyotype for girls and women with Turner syndrome. In some cases, only part of one sex chromosome has been lost. Such girls have 46 chromosomes, but one of their X chromosomes is incomplete. An indication of the shape of the incomplete chromosome will then appear in their karyotype - eg 46, XrX, 46, XdelXq, 46, XiXq and the like. We refer to this condition as a "structural anomaly" or a deviating shape of the "X" chromosome. Girls with a structural X chromosome anomaly also have Turner syndrome.
Other girls or women with Turner syndrome have a "chromosomal mosaic" - a mixture of two or more different sets of chromosomes. In them, when the eggs and sperm fused, the set of chromosomes was perfect, but during one of the other cell divisions, one or part of the "X" chromosome was lost. These girls most often have a part of cells with karyotype 46, XX and another part with karyotype 45, X (45, X / 46, XX). The proportion of individual cell lines can be expressed in percentages. In practice, however, this is not important because the proportion of these cells in the blood, where the karyotype is usually examined, may not be the same as their proportion in important organs of the human body.
All of these groups of women and girls have Turner syndrome. Whether they have karyotype 45, X, a structural anomaly of the "X" chromosome or a chromosomal mosaic. Their problems are basically the same. We will therefore continue to talk about all of them together.

Giant. 1: Different karyotypes (chromosome assemblies) in Turner syndrome.
All three groups of girls and women have similar symptoms.
In particular, they have in common smaller stature and, for most, ovarian dysfunction.
We are still talking about women and girls. Men don't have Turner syndrome. If the X chromosome is lost in the chromosomal assembly and karyotype 45, Y is formed, the human embryo cannot develop further. There will be an early abortion. Human life without an "X" chromosome is not possible.
Exceptionally, in some girls, the male sex chromosome "Y" or a fraction thereof, usually in the form of a chromosomal mosaic, may be found in the karyotype in addition to the "X" chromosome. Most of these girls also have symptoms of Turner syndrome. However, we need to pay more attention to their gonads, as we talk about in the ovaries section.
How did Turner syndrome get its name?
In 1938, the American physician Herna Turner noticed that seven of his patients had some common characteristics: a small figure, a lack of pubertal development, a pterygium colli, a lower hairline at the back of the neck, and a limited ability to stretch the arms in the neck. elbow joints in a straight line ("cubiti valgi"). He published his observations in a well-known medical journal, and in his honor, this set of symptoms was referred to as "Turner's syndrome." Much later, in the 45s, when it was already possible to reliably examine the karyotype, this examination was actually performed on one of Henry Turner's former patients and karyotype XNUMX, X was found. In Germany, Turner syndrome is referred to as "Ullrich-Turner syndrome" in honor of the German physician Dr. Ullrich, who noticed for the first time a similar set of symptoms in a German girl. In Russia, for similar reasons, it is called "Turner-Shereshevsky syndrome".
Can Turner syndrome be prevented?
No one is to blame for Turner syndrome. The loss of the "X" chromosome or part of it is, as we know today, a random whim of nature. The onset of Turner syndrome does not depend on the mother's age or the health or habits of the parents. The mother's behavior during pregnancy with Turner syndrome is by no means related, because it was decided earlier, at the very beginning of the little man's development - when fertilizing an egg with sperm.
Turner syndrome does not occur more often in certain families. A family who already has a baby girl with Turner syndrome has no increased risk of developing it in the next pregnancy.
Therefore, the onset of Turner syndrome cannot be prevented.
How can Turner syndrome be detected?
Although in some girls the manifestations of Turner syndrome can be so conspicuous that the doctor already has an urgent suspicion during a routine examination, it is always necessary to examine the assembly of chromosomes in the cell nucleus for the definitive determination of Turner syndrome, karyotype.
The karyotype is most often examined in lymphocytes, one group of white blood cells. These can be easily obtained by taking blood. In the laboratory, these blood cells are allowed to grow - they form a "cell culture". At some stage in the growth of this cell culture, when the chromosomes are clearly visible, they are examined under a microscope and photographed. The chromosomes are cut out of the photograph, sorted into pairs, and found to be complete. In this way, at least thirty, but preferably more cells should be examined. The diagnosis of Turner syndrome is characterized by the absence or imperfect formation of one X chromosome in at least 5% of all cells examined. Usually, however, there are significantly more cells with an X chromosome disorder or all of them are affected.
In some cases, the result of the karyotype examination from lymphocytes may be questionable or still needs to be clarified. It may then be necessary to examine the karyotype of skin cells called fibroblasts. They are obtained by miniature collection of skin particles by skin biopsy.
The karyotype doesn't change during a person's lifetime. One reliable karyotype examination is sufficient for the diagnosis of Turner syndrome.
How common is Turner syndrome?
Turner syndrome affects one in 2000 to 2500 girls and women. In the Czech Republic, an average of 20-25 girls with Turner syndrome are born every year. In total, we have about 2000 women with Turner syndrome.
After finding out Turner syndrome, parents often think that they are alone with their problem, that they are abandoned in the middle of the parents of other, healthy girls. However, the relatively high incidence of Turner syndrome suggests that there are about 50 girls and women living in a city of 000 who have Turner syndrome themselves.
2. Turner's syndrome before birth
Turner syndrome can be detected during pregnancy. This is possible if the mother had a placenta sample (chorionic villi biopsy) or amniotic fluid sample (amniocentesis) or umbilical cord blood sample (cordocentesis) taken for genetic testing in the first half of her pregnancy for another reason. Turner syndrome may be an accidental finding in such an examination.
After such an examination, the parents have the right to decide for themselves whether they wish to terminate the pregnancy or continue it. Before making their decision, they should be familiar with Turner syndrome and realize that living with Turner syndrome has some complications, but that the vast majority of girls and women with Turner syndrome can live a rich and happy life.
Theoretically, it would be possible to detect Turner syndrome before birth in this way in all families. But it would mean subjecting all mothers to a demanding and burdensome examination, which is not possible in practice.
Exceptionally, Turner syndrome can be detected during pregnancy and by ultrasound. This harmless test is being performed today for all future mothers. However, it is unreliable for the detection of Turner syndrome.
3. Newborn baby girl with Turner syndrome
Girls with Turner syndrome tend to be born a little earlier and tend to have a slightly lower birth weight. However, this is not the rule - and even in this case, the date of delivery and birth weight usually do not deviate from the broader norm.
Swelling (lymphedema)
In some girls with Turner syndrome, swelling of the legs, especially the insteps, and hands (lymphedema) may be noticeable after birth. They arise because the fetus does not have enough small lymph vessels to drain fluid from the soft parts of the body back into the blood.
These swellings usually disappear within half a year or one and do not cause any problems. Only in exceptional cases do they last longer. However, after birth, they can bring doctors on the trail of Turner syndrome.
Skin fold on the neck (pterygium colli)
Another striking sign may be the skin lashes on the sides of the neck in some girls, which create the impression of a wide neck (pterygium colli). They have a similar cause: In intrauterine life, the tissue fluid settled in the neck area because it could not drain well. Pterygium colli does not cause any health problems. If the girl decides later in childhood or adolescence to surgically remove excess skin lashes for cosmetic reasons, it is possible to consult a specialized plastic surgery department.
Heart and blood vessels
Girls with Turner syndrome are more likely than other children to have a congenital heart or large blood vessel defect. Some heart defects appear in the first days of life, others are found out only during a targeted ultrasound examination of the heart. Every girl with Turner syndrome should have that. Almost all congenital heart defects can be successfully operated on today. If the baby has a good heart after birth, the parents no longer have to worry. Later in life, a heart defect will not arise.
In the case of finding a congenital heart defect or large blood vessels, girls with Turner syndrome are taken on by a heart disease specialist - a pediatric cardiologist.
Kidneys
The kidneys and urinary tract can also be somewhat different in Turner syndrome. The so-called "horseshoe-shaped kidney" is relatively common, when both kidneys at their lower poles are connected in the shape of a horseshoe.
These deviations only present exceptional difficulties. Nevertheless, every girl with Turner syndrome should undergo an ultrasound examination of the kidneys. Deviating kidney formation can, in some cases, make urine flow more difficult and promote a urinary tract infection. Regular investigation can detect and treat such complications in a timely manner.
Nails
Some girls with Turner syndrome have less usually shaped toenails, sometimes toes. They can be flat or turn sideways (cup-shaped nails). When cutting nails, it is good to be extra careful in this case.
Failure
Some girls with Turner syndrome have feeding problems in the first year of life - they suck less (the cause may be a more arched floor), chew and swallow, sometimes they may be more prone to vomiting or blinking than other children. Due to frequent vomiting, they may then gain poor weight. These problems usually go away before the end of the first year and do not cause any problems in the next life.
4. Turner syndrome in childhood
Grow
Not all of the above-mentioned manifestations of Turner syndrome are present in many girls - or they do not have to attract attention. Most girls with Turner syndrome benefit as well as other children and do not have noticeable health problems. Therefore, Turner syndrome often occurs later in childhood. The most common reason for finding Turner syndrome at this age is growth failure.
All girls with Turner syndrome grow more slowly than other children. The delay in growth is often noticeable in the first years of life, but it becomes more and more significant as the years go by. Already when they start school, girls with Turner syndrome are on average 17 cm smaller than other girls of the same age. Young women with Turner syndrome grow to an average height of 146 cm when left untreated. This is exactly 20 cm less than the average adult height of Czech young women. If a girl with Turner syndrome has tall parents, she can grow to a height of 158 cm and will therefore not differ in size from small girls without Turner syndrome. However, if she did not have Turner syndrome, such a girl would grow to a height of 178 cm. Conversely, the daughter of a young parent who has Turner syndrome can reach only 134 cm in some adult cases (instead of 154 cm if she does not have Turner syndrome).
Adult height of untreated women with Turner syndrome
ranges from 134 to 158 cm (diameter: 146 cm)
We still do not understand the reason for the small stature of girls with Turner syndrome. We know that these girls produce normal amounts of growth hormone in their bodies, but their growth hormone is not enough to ensure normal growth. The long bones of the limbs, which make a decisive contribution to growth throughout childhood, are less sensitive to growth hormone in girls with Turner syndrome.
For many years, therefore, it was thought that low height was the inevitable fate of every girl and woman with Turner syndrome and that she could not be affected by treatment. It was not until the late XNUMXs that the first promising reports emerged, suggesting that high-dose therapeutic administration of growth hormone could at least partially overcome the low susceptibility of long bones to growth hormone. Thus, another growth hormone began to be added to the growth hormone itself as a drug.
We now know that growth hormone therapy really helps girls with Turner syndrome. Although it cannot completely eliminate the growth disorder, it can significantly alleviate it and allow the vast majority of girls to reach socially acceptable body height on the threshold of adulthood. Since 1991, when growth hormone therapy was started in girls with Turner syndrome in the Czech Republic, it has been given to over 170 girls. Each year of treatment will help a little, but only long-term, long-lasting treatment brings the greatest benefit.
| diameter | range | |
|---|---|---|
| without growth hormone treatment | 146 cm | 134 - 158 cm |
| if the treatment lasted 1 year | 149,8 cm | 137,8 - 161,8 cm |
| if the treatment lasted 2 years | 151,9 cm | 139,9 - 163,9 cm |
| if the treatment lasted 3 years | 153,2 cm | 141,2 - 165,2 cm |
With each passing year of treatment, adult height continues to improve somewhat.
Growth hormone treatment is quite demanding. It is performed at selected pediatric clinics that have sufficient experience with this treatment. There are twelve such places in the Czech Republic. You can ask your pediatrician to see a specialist in growth hormone treatment.
Growth hormone is given by injection. It is a substance of a proteinaceous nature which, when administered in tablets, drops or syrup, would be disturbed by the digestive juices in the digestive tract and only its ineffective residues would pass into the blood. Therefore, the digestive system must be bypassed during treatment.
Growth hormone injections are given subcutaneously. This easiest way to give injections is easy for anyone to learn. Parents and older girls themselves will soon gain such skill in injecting that stinging is no bigger problem for them than brushing their teeth. In order for the body to benefit most from growth hormone, it needs to be given every day. The best time to inject is at bedtime. The reason is the fact that in every child, the growth hormone in the body is most produced in the first hours of the night after falling asleep, and the natural rhythm of the action of the growth hormone is faithfully imitated by injection before going to bed. In addition, we have enough peace to inject the night before bed, and if it becomes part of our daily evening activities, we will not forget it.
Growth hormone injections are almost painless. Special pens with a very thin needle are available for administration, which everyone can easily learn to operate.
Growth hormone therapy is always voluntary in girls with Turner syndrome. The decision to start treatment is the joint conclusion of the parents and the doctor. Parents should always be well informed before making their decision. They should understand the patterns of growth in girls with Turner syndrome and know that if the growth disorder is not yet noticeable in preschool age, it may be much more noticeable later, eg at the age of twelve - but delaying treatment has uncomfortably shortened the time the girl will grow and the overall effect of the treatment will no longer be ideal. The doctor should always acquaint the parents with the predictions of the adult height of their daughter. Such a prediction is not entirely accurate, but it will help for orientation.
We know from experience that most parents choose growth hormone therapy. Sometimes the purpose of treatment is considered by tall parents, whose daughter with Turner syndrome has a chance to grow up to a height of 158 cm without treatment. Parents may consider this adult height to be sufficient. However, even such a girl will grow more in the case of growth hormone treatment.
Many parents of girls with Turner syndrome ask about possible side effects before starting growth hormone treatment. Growth hormone is a substance in the body. As a drug, it is produced in a way that ensures that the final product is completely identical to its own growth hormone. From this point of view, treatment is safe.
The fact that we give more growth hormone than usual for the human body can be a problem. Indeed, increased amounts of growth hormone can have some side effects. However, from the experience of more than 170 girls treated to date in the Czech Republic, we can state that these side effects are not dangerous - and so far have not led to the need to interrupt treatment.
One of the possible side effects of growth hormone treatment is the retention of more water in the body. This usually does not lead to difficulties. However, if the girl had swelling of the insteps or hands (lymphedema) after birth, a sign of swelling may reappear after starting treatment. However, they only rarely cause greater problems.
It is also necessary to monitor the maintenance of blood sugar (glycemia) during growth hormone therapy. Your doctor will take responsibility for regular check-ups in this area (examination of so-called glycosylated hemoglobin, HbA1c). Girls with Turner syndrome are born with a slightly increased tendency to develop diabetes, and in some, mild diabetes actually manifests itself in adulthood. Growth hormone is known to increase the tendency to develop diabetes in some cases. Initially, therefore, we closely monitored all girls with Turner syndrome during growth hormone treatment. However, the experience is encouraging. An increased incidence of diabetes during growth hormone treatment has not been observed in our country or in other countries.
According to previous experience, growth hormone treatment in girls with Turner syndrome is therefore not only effective but also safe.
Hearing
Some girls with Turner syndrome may have noticeably frequent otitis media. The cause is a slightly deviating curvature of the Eustachian tube, which creates a connection between the middle ear cavity and the nasopharynx. In girls with Turner syndrome, even with small inflammation of the nasopharynx, the Eustachian tube may become temporarily blocked. An impenetrable Eustachian tube causes the feeling of a "lying ear" and impairs hearing. At that time, otitis media often begins to develop, which can lead to perforation (rupture) of the eardrum.
Often recurrent or lingering otitis media can cause long-term or even permanent hearing loss. Therefore, especially for girls with Turner syndrome, it is very necessary that their otitis media be recognized in time and treated thoroughly. Although we usually do not advise using antibiotics too often, it is always better to use antibiotics in order to manage the inflammation as soon as possible and to reduce the risk of its transition to a prolonged stage.
A little girl with Turner syndrome who has problems with otitis media should be monitored by a specialist ear doctor (otorhinolaryngologist) who has sufficient experience with similar children. Hearing impairment is not inevitable and can often be prevented by proper treatment.
Exceptionally, hearing loss in a girl with Turner syndrome may be congenital. That is why it is beneficial if the examination for Turner syndrome also includes an audiogram - an examination in which even a slight hearing loss can be recognized, even at certain pitches. Unrecognized and untreated hearing loss brings problems in speech development, later it can be one of the causes of school failures. At the same time, it is easy to face.
Air
Myopia or squinting occur in many children. They are only slightly more common in Turner syndrome, but they are treated similarly to other girls. If we recognize them in time, we will prevent further problems. Therefore, every family of a girl with Turner syndrome should have the opportunity to visit a specialized pediatric ophthalmologist (ophthalmologist).
Exceptionally, a decrease in the upper eyelids (ptosis) may also occur. It can impair visual well-being, forcing the head to tilt. Eyelid ptosis can be treated with plastic treatment.
Skin
Some girls with Turner syndrome have prominent pigmented spots (nevi) on their skin. Their number may increase slightly during growth hormone treatment. The development of large nevi should be monitored by a specialist in skin diseases - a pediatric dermatologist.
5. Girl with Turner syndrome at school
What are the mental abilities of girls with Turner syndrome?
By comparing the mental abilities of girls with Turner syndrome with their sisters, they were found to be completely intellectually comparable. This refuted a long-held prejudice about reduced mental abilities in Turner syndrome.
Girls with Turner syndrome perform better in intelligence tests in the verbal (verbal) component than in non-verbal (written, cartoon or mathematical) tasks. Their weaker side may be the lack of concentration and a somewhat worse spatial imagination, which is needed in solving mathematical problems.
How are they doing at school?
Most girls with Turner syndrome are successful at school. As with other children, the pupils are above average, average and below average.
However, for many of them, some features are common: They often learn to read earlier than other children, but the age at which they begin to write is a little later. Solving problems associated with spatial imagination, especially mathematical and geometric, can be a certain weakness. Teachers should be informed. However, they should not underestimate the girl and consciously place less demands on him than on others.
What are their relationships with classmates?
Due to their supportive nature, girls with Turner syndrome tend to have many friends at school and beyond, and are often very popular with classmates.
Are some character traits typical for them?
Typical character traits of girls with Turner syndrome include openness, diligence and zeal, conscientiousness, non-moodiness. Girls with Turner syndrome have a sense of order and take great care of their appearance, which is reflected in care in dressing, styling or facial hair.
A certain immaturity in the emotional area can accompany a girl with Turner syndrome through childhood and adolescence. She becomes an "adult" a little later than her classmates. Sometimes also because her family and surroundings consider her younger than she really is (mainly because of her smaller figure) and they try to "protect" her for longer. This approach does not contribute to the development of self-confidence, slows down emotional maturation, increases the girl's dependence on the family and thus, especially in adolescence, isolates her somewhat from her peers and assigns her to younger children. It will help a girl with Turner syndrome if her family, teachers and friends treat her appropriately at the level of her age and not her height. This also applies to dressing, involvement in extracurricular activities, requiring a certain degree of responsibility for the tasks performed and the like.
Recently, thanks to growth hormone treatment, which improves the height of girls, we encounter these problems less. They are mainly those in girls who have been diagnosed with Turner's syndrome late or who have not been started on growth hormone therapy.
Katka's mother, who has been going to our surgery since she was 9 years old, says: "Katka always had a lot of friends, but especially among younger children. I was happy because I thought she was happier among them. Interestingly, she always had a leading role in the group and was able to take good care of younger children, even though she looked just as old. When Katka went to the first grade and the pediatrician recommended postponing school attendance, we consulted a child psychologist, who disagreed. She started isolating herself from her classmates, and she missed a lot because she had recurrent otitis media, and she even had to be admitted to the hospital, where the doctor told me that she suspected our daughter had a genetic disorder. That it was not a disease, but rather a set of symptoms caused by the absence of a single chromosome. will continue. We kept asking new and new questions. The doctor talked to us repeatedly and for a long time - about further examinations, treatment, adolescence, adulthood. Very soon, Katka began treatment with growth hormone. During the first year of treatment, it grew almost 8 centimeters. Suddenly, we all watched in surprise as she became confident, joined her classmates, and even joined the Scout Squad. She is now almost 14 years old, one of the better students at the school and she would like to study at a medical school where she will not need so much math. He leads a scout unit, has a lot of friends and is no longer the smallest in the class ... "
Katka's mother told this story not only for herself, but for many other parents of girls with Turner syndrome.
6. Turner syndrome in adolescence
Adolescence (puberty) is the period when a child is born into an adult.
At the beginning of adolescence, the gonads (ovaries in girls) begin to produce sex hormones (estrogens in girls, later progesterone). Puberty begins with individual girls of different ages, usually between the ages of 9 and 13. The production of female sex hormones is initially small, but continues to increase during adolescence. Due to sex hormones, girls typically experience changes in their body shape. Growth accelerates, the mammary glands develop, the uterus and vagina enlarge, the pelvis widens, and adipose tissue begins to accumulate in typical landscapes of the body. At the peak of adolescence, the first months appear, which signals the beginning of regular (cyclical) production of hormones, which leads to the separation of the uterine mucosa at an interval of approximately 28 days, accompanied by bleeding (menstruation), lasting 3-5 days. All of these changes begin gradually, usually over 2-4 years.
The ovaries are therefore needed for development during adolescence. They produce female sex hormones and contain the base of eggs needed for future pregnancies. Little girls with Turner syndrome have normal-looking ovaries in the first months of their intrauterine life. Gradually, however, they begin to change and in most cases, they are unable to produce hormones or contain eggs. Therefore, the usual changes do not occur at the time of the expected onset of puberty. An exception is a small number of girls, who usually have a chromosomal mosaic in the karyotype. Their ovaries may work for a period of time, they may develop normal adolescence and may even have regular periods, and in rare cases may become pregnant.
With the exception of the ovaries, the internal and external genitalia of girls with Turner syndrome are completely normal.
Missing ovarian hormones can be replaced with appropriate drugs. Thanks to this, it is possible to induce puberty perfectly and maintain female maturity, including a regular menstrual cycle. This task is usually performed by a pediatric endocrinologist, later treated by a gynecologist.
When is the best time to start growing up?
During adolescence, a person is much more sensitive to his surroundings. The girls just want to be as well informed as possible about how their hormonal treatment will take place and what they can expect in the near future.
As we already know, individual girls without Turner syndrome begin to grow at different ages. Therefore, even for a girl with Turner syndrome, it is necessary to carefully choose the time when the induction of adolescence will be most appropriate. It is necessary to assess a number of circumstances and discuss them in detail with the girl and her parents, so that we do not rush the beginning of adolescence unnecessarily or delay it inappropriately. Estrogens given prematurely are known to shorten overall growth time and thereby reduce adult height. They lead to the closure of growth cracks in the long bones. Therefore, we recommend starting the administration of female hormones a little later. The appropriate time is not the same for all girls and can be determined from an X-ray of the wrist. Your doctor will tell you when it will be appropriate to start estrogen treatment so that the adult height suffers as little as possible. While we start growth hormone treatment as soon as possible, we usually postpone estrogen administration between the ages of 13 and 15. The reward is a gain of a few extra centimeters in height, at the cost of a slightly later shaping of the figure in a female direction. If a girl and her parents decide to grow up earlier, their views will be respected. Usually, however, girls with Turner syndrome do not rush into adolescence because they know classmates who also start growing up later.
We'll talk about treatment female sex hormones, but in reality it is not a cure, but a substitute for substances that the body cannot produce. The doses of female sex hormones are therefore very low at the beginning and are gradually increased very slowly (over 2-3 years) in order to mimic their natural production in other girls.
We start with the administration of estrogens alone. Gradually, breasts will begin to develop, subcutaneous fat will accumulate in typically female areas (buttocks and thighs), and sometimes a whitish discharge will appear, which may be a harbinger of the approaching first period. When the first bleeding occurs, your doctor should be informed immediately, as this is the time when hormonal treatment needs to be adjusted. To maintain a regular menstrual cycle, it is then necessary to combine the female hormones estrogen (given in the first half of the cycle) with another female hormone called progesterone (given in the second half of the cycle). As soon as a dose of hormones is found that suits the girl and during which she has regular and heavy menstruation, this treatment is left for a long time. It used to be recommended to take hormone replacement therapy until you were about 50 years old, but now we know that small doses of female sex hormones are beneficial even longer. Estrogens also have a protective effect on the heart and blood vessels and improve the storage of calcium in the bones. Therefore, their use is also recommended for other adult women after menstruation (after menopause). There are several products containing female sex hormones and they exist in various forms. The most common are pills, but it is also possible to use patches from which the hormone is absorbed through the skin. Each form has its advantages and disadvantages. All are usually well tolerated and have no major side effects. They are very similar to hormonal contraceptives used by millions of women around the world. Exceptionally, headache, stomach pain, water retention or chest tightness may occur when administered. The gynecologist will recommend the appropriate combination, whether it is the type of product, the dose and the time of administration, and can change it at any time according to individual tolerance. Treatment must be continuous, uninterrupted to achieve balanced hormonal levels, regular menstrual cycles and proper uterine size. The administration of female sex hormones also leads to the production of vaginal mucus and thus enables a completely natural sex life.
Every girl should keep her menstrual calendar. It records the period of menstruation, its abundance and possible difficulties - abdominal pain, headache, discharge and the like. The menstrual calendar can be obtained free of charge at any gynecologist's office, sometimes a pediatrician, endocrinologist or pharmacy. It belongs in the purse of every modern girl and woman.
Young girls often ask if regular gynecological examinations are necessary during treatment with female sex hormones. We usually recommend them about 1-2 years after starting the combination treatment, especially to make sure that the development of the genitals corresponds to age - previously only in case of severe problems. The good effectiveness of hormonal treatment can be assessed primarily by the degree of development in the female direction, by regular menstruation and by monitoring the levels of hormones in the blood. Sometimes it is useful to perform a painless ultrasound examination.
If the ovaries do not fulfill their function, is it not better to remove them?
Surgical removal of the ovaries is only recommended for girls who have a Y chromosome or part of it in their karyotype. In their exceptional case, they could start developing in the ovaries in an undesirable, detrimental direction. The most reliable methods of examining a blood cork test, which are becoming available in the departments of medical genetics, are used to determine whether a girl has this karyotype. The examination can be arranged by your doctor.
If a small fraction of the Y chromosome is detected, we recommend removing the ovaries. This is a simple operation, but it should not be postponed. There is no risk after the operation. Hormonal treatment is then conducted as in other girls, and the development is clearly moving in a female direction.
A common concern of parents, and at a later age of the girls themselves, is whether they are women in the true sense of the word, even if they lack one or part of their sex chromosomes. It is appropriate to reassure them that their feelings, temperament and behavior are purely feminine. Their relationship with the opposite sex is reasonable, only sometimes it can be affected by a certain emotional immaturity, which can be reflected in the establishment of partnerships and the later beginning of sexual life. It is usually full-value and is contributed to by normal levels of female sex hormones in the blood, whether produced naturally or supplied in the form of drugs.
7. Turner syndrome in adulthood
Parents help to solve most problems in childhood or adolescence. As an adult, a woman with Turner syndrome becomes independent and finds a partner. Some new problems are emerging, typical of adulthood. The care of paediatricians is ending and the young woman should find a specialist with their help who knows the issue of Turner syndrome well and will therefore not underestimate some problems or overestimate others unnecessarily. It will work with doctors in other fields, as it will be necessary to continue treatment initiated in childhood and adolescence, to monitor any previous associated medical abnormalities (such as hearing, vision, kidney and heart disorders), but also to face the difficulties that age can bring. adulthood. It is important that the care of a girl or woman with Turner syndrome is not interrupted, so that the woman is not left without "her doctor", whom she trusts.
Can a woman with Turner syndrome get pregnant?
We already know that the vast majority of girls and women with Turner syndrome do not have well-functioning ovaries. The role of the ovaries is both to produce female sex hormones and to release eggs into the fallopian tubes, which are ready for fertilization by the male germ cell - sperm. Therefore, most women with Turner syndrome cannot get pregnant naturally. Rare exceptions are women with chromosomal mosaics and most cells with karyotype 46, XX. However, even their possible pregnancy carries with it the risk of birth defects or chromosome disorders in the fetus, so it must be monitored both by a gynecologist and at a specialized workplace of medical genetics.
And what about other women who have a partner and long for a child?
There has been a possibility for several years artificial insemination (in vitro fertilization - IVF) sperm eggs outside the mother's body. This is how "children from the test tube" are created, of which thousands have already been born in the world. This procedure is often used in cases where a woman forms eggs but they cannot be fertilized in a natural way. The egg is taken with a special device and fertilized with the sperm of the woman's partner. At other times, this procedure can be used for male infertility - the collected egg is fertilized in the test tube with the donor's sperm. In all cases, the fertilized egg returns to the mother's uterus, and if it nests there successfully, the woman experiences a natural pregnancy.
At present, our laws allow not only the donation of male germ cells (sperm), but also the donation of eggs. The egg donor is an anonymous healthy woman who has no hereditary burden in the family. She undergoes an examination in a genetic clinic and is also examined for karyotype.
Such donated eggs can also be used for artificial insemination of a woman with Turner syndrome. They can also be fertilized in the test tube with the sperm of their own husband. The condition for successful nesting of a donated egg in the uterus of a woman with Turner syndrome is an adequate size of her uterus. Prior long-term and regular administration of female sex hormones is therefore essential. Pregnancy must be maintained by supplying hormones until their own placenta takes over. Throughout such a pregnancy, the woman is regularly checked - in addition to routine examinations, blood hormone levels, blood sugar levels (blood sugar), urine and blood pressure are monitored. The size of the fetus, its growth and development are checked by ultrasound.
Recently, the transfer of a donated egg has been preferred to spontaneous pregnancies even in those women with Turner syndrome who exceptionally make eggs. The reason is a lower probability of congenital malformation of the fetus. Each gynecological, genetic or endocrinological center will provide information on specialized centers for this type of artificial insemination. The success rate of egg transfer is currently between 25 and 30%.
For some women, artificial insemination is not suitable for health reasons, others reject it, for example for religious reasons, and for some they fail even after repeated attempts. The solution can then be one of the types adoption child (adoption or foster care). Information on adoption options will be provided by the attending physician or the substitute family care department at the city or district office. Both in artificial insemination and in the adoption of a child, a woman needs to be married or have a partner.
Osteoporosis
Osteoporosis can be one of the problems of women with Turner syndrome. By this we mean a gradual loss of calcium in the bones and a reduction in their strength. This problem affects most women in old age, but with Turner syndrome tends to come earlier. It was originally thought that the cause was the lack of female sex hormones. Today we already know that a different bone structure is also involved. Osteoporosis can cause unpleasant problems - pain or even more frequent fractures in minor injuries or sports.
How can osteoporosis be detected?
In recent years, there has been a very accurate and non-burdensome examination of bone mass. It's called densitometry, or measuring bone density. It resembles an X-ray, but does not expose a person to a significant dose of radiation. As a rule, the most congested areas of the skeleton, especially the lumbar spine, are examined.
Can osteoporosis be treated?
Growth hormone therapy alone in childhood has a positive effect on bone condition. It also helps to administer female sex hormones. Lifestyle also plays an important role. The diet should be rich in calcium, which is mainly found in dairy products. It can also be used in the form of tablets, sometimes a small dose of vitamin D is added to it. Regular recreational sports are very suitable for the prevention of osteoporosis.
Other health problems
It is more common in women with Turner syndrome higher blood pressure (hypertension). The cause can be both an unrecognized heart defect and congenital kidney defects or abnormal vascular formation. In some women, the cause of the higher blood pressure is not identified.
Tendency to higher blood sugar levels (higher glycaemia) is slightly more common in women with Turner syndrome than in other women. However, typical diabetes rarely develops. As a precaution, girls and women with Turner syndrome are advised not to overeat sweet and maintain optimal body weight. The slim figure in combination with appropriately chosen clothing and extra accessories seemingly adds a few extra centimeters to each woman.
It may be more common in women with Turner syndrome decreased thyroid function. This disorder does not hurt, but it can make life miserable because it reduces physical and mental performance. Healing is relatively easy. Therefore, it pays to check thyroid function once a year by blood sampling.
With increasing age, the tendency to wound heals increases stiffer (keloid) scars. This should be kept in mind by women who opt for plastic surgery, for example - drooping eyelids, skin lashes on the neck, pigmented nevi.
8. Is Turner syndrome a disease?
We don't consider Turner syndrome to be a disease. Rather, it is a set of symptoms and difficulties that are not permanent and can usually be successfully addressed. Congenital malformations (kidneys, heart, neck lashes and others) can be operated on and will no longer manifest for the rest of your life. Today, we also treat growth retardation and ovarian dysfunction, mostly with good results. The current young generation of girls and women with Turner syndrome will no longer face the problems that have plagued women in the past, when treatment options were still limited.
It is important to recognize Turner syndrome as soon as possible. It can not only be treated in time and therefore more successfully, but also soon and truthfully inform the parents and later the girl about the cause of her difficulties. It is the duty of the physician to provide comprehensive information and the duty of the parents or later of the girl or woman herself is to request further information. But not everyone finds the courage to ask openly during their first contacts. Some questions may seem unnecessary at first, others are embarrassing. This text should therefore also provide little help.
I AM ME
(Title track of Lenka Kosinová's CD of the same name - the first CD sung by a woman with Turner syndrome. The text was written by Ilona Rybářová.)
If I were the wind from the mountains,
what the dust tolerates in the valley,
the wind what he says
I would not be afraid from afar.
If only I could for a while
see the trees bloom in the sun
perceive the rainbow of butterflies,
I would be punished for that.
But I'm me,
so let me be no more
I have to give you strength
your love, otherwise nothing.
If I were a meadow in bloom,
where children go to play,
she whispered her songs to them,
she learned to know them.
If I were a river of stones,
the river that found the dam,
its power from the springs
I would spill you.
I'm me,
so let me be no more
I have to give you strength
your love
and with her I go to meet you.
Some prejudices that a girl or woman with Turner syndrome may encounter
Prejudice: Girls with Turner syndrome have a reduced intellect.
Explanation: It's not true. When comparing the intellectual abilities of girls with Turner syndrome and their sisters without Turner syndrome, they were found to have comparable intellect. Some girls with Turner syndrome may have certain mathematical difficulties due to their less spatial imagination. In other areas, however, other girls outperform, as we discuss in the relevant chapter.
Prejudice: Growth hormone therapy does not make sense because low altitude in Turner syndrome cannot be affected.
Explanation: It's not true. Reports of growth hormone therapy have been reported in the early XNUMXs, when completely inadequate doses were given. Currently, the beneficial effect of growth hormone treatment on adult height is clearly demonstrated.
Prejudice: A girl with Turner syndrome can't play sports.
Explanation: It's not true. Girls with Turner syndrome can be as successful in many sports as their classmates. The handicap can only be a smaller height, so it is appropriate to choose the sport judiciously.
Prejudice: Women with Turner syndrome do not have a natural sexual feeling.
Explanation: It's not true. Women with Turner syndrome have the prerequisites for establishing natural partnerships just like other women. They do not have increased homosexuality or other abnormalities. Sexual sensation in them is enhanced by the administration of female sex hormones, which is a natural part of ovarian function replacement.
Prejudice: A woman with Turner syndrome can never give birth.
Explanation: It's not true. The uterus develops in women with Turner syndrome in the same way as in other women, and thanks to the administration of female sex hormones, it also reaches its usual adult size. After transferring a fertilized egg to the uterus (artificial insemination, in vitro fertilization), a woman with Turner syndrome can experience pregnancy and give birth.
Usual medical monitoring and treatment of girls and women with Turner syndrome
When detecting Turner syndrome:
- ultrasound examination of the heart and large vessels (echocardiography)
- ultrasound examination of the kidneys and urinary tract
- ear and eye examinations
- examination of thyroid function (blood sampling)
- growth and adult height prediction
- joint decision of the doctor and parents on growth hormone treatment
During growth hormone therapy:
- growth rate controls
- regular thyroid function tests (blood sampling)
- elimination of diabetes (blood sampling)
Before the usual age for adolescence:
- determination of ovarian function (blood collection)
- determination of bone maturity (X-ray of the wrist)
- decision on treatment with female sex hormones (gynecological examination is not necessary)
In adulthood:
- usually permanent treatment with female sex hormones (in the care of a gynecologist)
- regular thyroid function tests (blood sampling)
- elimination of diabetes (blood sampling)
- blood pressure monitoring
- monitoring of bone strength
More detailed examination may be needed for girls who have been found to have deviating findings or who have other health problems.
Glossary of technical terms
amniocentesis - amniotic fluid collection during pregnancy for genetic testing
autosomes - chromosomes that look the same in women and men
cubiti valgus - limited ability to stretch the arms at the elbows in a straight line
densitometry - bone density measurement
echocardiography - ultrasound examination of the shape and structure of the heart
estrogens - An important group of female sex hormones that are produced in the ovaries
Jan - the chemical structure in which the hereditary (genetic) information is recorded
heterochromosomes (gonosomes, sex chromosomes) - chromosomes that determine a person's gender. A pair of sex chromosomes XX is typical for women and XY for men. Girls with Turner syndrome often have only one X chromosome
hormone - chemical messenger inside the human body. It transmits information from the place of its origin to the so-called target tissues, the activity of which it regulates
chromosome - a unit in the cell nucleus that contains genes
chromosomal mosaic - a mixture of two or more different sets of chromosomes in cells of the same human
in vitro fertilization (IVF) - artificial insemination of an egg with sperm outside the mother's body. The egg is then fed back into the mother's uterus
karyotype - a set of chromosomes in the nucleus of every cell in the human body. Karyotype testing is necessary to diagnose Turner syndrome
aortic coarctation (narrowing of the heart) - congenital abnormality, which may occur in some girls with Turner syndrome. Narrowing is a barrier to blood flow to the lower half of the body, and the heart must work hard against high resistance. Aortic coarctation can be operated on
cordocentesis - collection of fetal umbilical cord blood during pregnancy for genetic testing
lymphedema - swelling in case of insufficient outflow of tissue fluid (sap, lymph). In Turner syndrome, lymphedema can affect the backs of the hands and insteps. They are usually transient and disappear during the first year of life
osteoporosis - loss of calcium in the bones and reduction of their strength
placenta - fruitcake. The organ inside the uterus through which the fetus receives oxygen and nutrients from the mother's body. Also the place of origin of hormones important for the course of pregnancy
horseshoe kidney (ren arcuatus) - congenital kidney disease, which occurs in some girls with Turner syndrome. He only rarely causes difficulties
progesterone - one of the female sex hormones
pterygium colli - skin fold (doubling of the skin) laterally on the neck. May give the impression of a wide neck.
ptosis - drop of upper eyelids
puberty - adolescence. The birth of a child into an adult
sperm - mature male germ cell
syndrome - set of flags
structural anomalies - deviating shape
ultrasound (sonography, ultrasonography) - examination method in which the internal organs of the human body are imaged on the principle of ultrasonic waves. Completely painless and harmless examination
egg - mature female germ cell
Specialist doctors a girl and a woman with Turner syndrome may encounter
allergist - specialist in the treatment of hypersensitivity diseases
endocrinologist - specialist in the treatment of hormonal disorders. He usually coordinates the care of a girl and a woman with Turner syndrome
dermatologist - specialist in the treatment of skin diseases
gastroenterologist - specialist for the treatment of diseases of the digestive system
genetic - specialist for the detection of hereditary and congenital diseases. Significantly involved in the diagnosis of Turner syndrome
gynecologist - specialist for the treatment of diseases of the female genital organs
cardiologist - specialist in the treatment of cardiovascular diseases
nephrologist - kidney disease specialist
ophthalmologist - specialist in the treatment of eye disorders
otolaryngologist - specialist for the treatment of diseases and disorders of the ears, nose and larynx
urologist - specialist in the treatment of urinary tract diseases
History of Turner syndrome in data
1768
Dr. Giovanni Battista Morgagni, considered the father of the scientific conception of medicine, described in a deceased woman in whom he performed an autopsy, symptoms resembling Turner syndrome - small stature, deviating kidney formation and lack of ovarian tissue. His findings have been overlooked by the medical community for more than 150 years.
1883
Dr. Kobylinski described a male patient with lashes on his neck. For many decades, this has called into question the true nature of Turner syndrome, which only affects women.
1902
Dr. Funke published the observations of a 15-year-old girl with a small figure, lack of adolescence, skin lashes on the neck, swelling of the legs, but also other manifestations of Turner syndrome - low-set ear lobes and a high, arched palate.
1929
Dr. O. Ullrich reported at the Munich Society of Pediatrics about an eight-year-old girl with symptoms of Turner syndrome. Therefore, in Germany, Turner syndrome is still called Ullrich-Turner syndrome.
1938
Dr. Herny Turner, an internist in Oklahoma City, wrote an article in a reputable trade magazine describing more girls and women with symptoms of Turner syndrome. He has been bearing his name ever since. Later, Dr. Turner pioneered the administration of female sex hormones to these women. For the first time, they could be helped effectively.
1959
Dr. Ford has developed a method for examining karyotypes and has shown that the absence of X chromosome is the cause of Turner syndrome.
1970
Dr. Turner died at the age of 78.
1981
The first Turner Syndrome Society was formed in Toronto, Canada. Its aim was to spread knowledge about Turner syndrome among the families of affected girls, among adult women with Turner syndrome, but also among the medical community. Today, Turner Syndrome companies or clubs exist in many dozens of countries around the world, providing empowerment and assistance to thousands of Turner Syndrome carriers.
1985
The first woman with Turner syndrome became pregnant thanks to a donated egg.
1986
Research into the effectiveness of growth hormone therapy in Turner syndrome has begun in the United States and Europe.
1989
The Club of Girls and Women with Turner Syndrome was founded in Prague. Its members are girls and women from all over the Czech Republic. Club address: 160 00 Prague 6, Kladenská 1.
1990
The club started publishing the magazine "Téčko".
1991
Launch of the first Czech study with growth hormone in ten girls with Turner syndrome.
1992
Growth hormone treatment has become available to girls with Turner syndrome throughout the Czech Republic.
1996
Lenka Kosinová's CD "I am me" is released - the first CD sung by a woman with Turner syndrome.
1997
The first woman with Turner syndrome in the Czech Republic gave birth to a baby from a donated egg.
1998
Lenka Kosinová is preparing the release of the second CD entitled "Stay on top of things"
Authors
Prof. MD Jan Lebl, CSc. (born 1955) is the head of the Pediatric Clinic of the 2nd Medical Faculty of Charles University and the University Hospital in Prague-Motol. He graduated from the Medical Faculty of Charles University in 1980. He defended his dissertation on "Diagnosis of children with growth disorders" in 1990 and the habilitation thesis "Treatment with growth hormone" in 1993. He cares for children with growth and development disorders, diabetes and other endocrine diseases. In 1989, he initiated the establishment of the Club of Girls and Women with Turner Syndrome. In the early 1996s, together with other Czech and Moravian pediatric endocrinologists, he was responsible for the introduction of growth hormone therapy in these girls. He is the author of the monograph "The Growth of Children and Its Disorders" (1997), several books for parents ("The Growth and Maturation of Your Child" - XNUMX and others) and many articles in the professional press. It emphasizes the patient's active approach to his health problem. He is a supporter and promoter of the idea that parents and children should be well informed about their health, should understand it well, and should be able to choose a doctor who will provide them with care at the level of current medical science.
Contact adress: Department of Pediatrics, Charles University, 2nd Faculty of Medicine and University Hospital Motol, V Úvalu 84, 150 06
Prague 5Doc. MUDr. Jirina Zapletalova, Ph.D. (born 1954) is an associate professor at the Children's Clinic of the Medical Faculty of Palacký University in Olomouc. She graduated from the Medical Faculty in Olomouc in 1979. She has been involved in pediatric endocrinology for over twenty years, and has been specializing in the treatment of children with growth and adolescence since the mid-2003s. She is one of the most active members of the Working Group for Growth Hormone of the Czech Endkorinological Society, is a member of a number of domestic and international medical societies (eg Growth Hormone Research Society) and represents the Czech Republic in the KIGS international growth study committee. She has lectured at home and abroad and published a number of articles in professional literature. She is the main author and organizer of the first Czech monograph on Turner syndrome, which was published in XNUMX.
Contact adress: Department of Pediatrics, University Hospital, IPPavlova 6, 775 20 Olomouc
Premature adolescence
Download full text: Premature adolescence [doc; 603 kB]
Home
Premature adolescence is a general term encompassing not only premature puberty but also other disorders. We talk about it when the development of sexual characteristics begins in girls before the age of 8 (development of breasts, genitals or pubic hair = hair around the genitals) or axillary hair (underarms) and 9 years ago in boys (development of genitals, hair).
This text was created to help you understand both normal and premature adolescence and their variants. It will help you get acquainted with some medical terms, with treatment and with the possibility of family participation in the treatment.
Control of hormone production in the body
Hypothalamus is the part of the brain that is located above the pituitary gland, the hypothalamus is connected to the pituitary gland by a so-called stalk. With the help of regulatory hormones, the hypothalamus has a controlling - regulatory significance for the release of hormones of the anterior pituitary gland. The hypothalamus also produces a hormone that regulates water absorption in the kidneys and a hormone related to childbirth and lactation (to the production of breast milk).
Hypophysis or brainstem is a gland the size of a pea. This gland is often referred to as the "master gland." A number of hormones are formed in its anterior lobe, which are essential for the control of hormonal production in other endocrine glands. It is a growth hormone, hormones that control the function of the thyroid gland, adrenal glands or gonads. The posterior lobe of the pituitary gland serves as a reservoir for other hormones that are formed in the hypothalamus (a hormone that regulates water absorption and a hormone related to childbirth and lactation).
Hormones
They are chemicals released into the blood from the relevant endocrine glands. Their function is to transfer information between cells and maintain normal bodily functions. Many hormones are produced in the body: for example, the already mentioned thyroid hormones, growth hormone, sex hormones, adrenal hormones, insulin and others. The following hormones control adolescence (or puberty):
GnRH
gonadotropin releasing hormone (hormone releasing gonadotropins) is formed in the hypothalamus, controlling the production of hormones called gonadotropins. We also discuss gonadotropins elsewhere. Gonadotropin releasing hormone plays a key role in controlling puberty and fertility.
Gonadotropins
is formed in the cerebral cortex under the controlling influence of GnRH (gonadotropin releasing hormone). These are hormones called FSH and LH.
FSH: or follicle stimulating hormone supports the testes to produce male germ cells (sperm) and ovaries to develop female germ cells (eggs, oocytes) and together with luteinizing hormone supports the production of female sex hormones.
LH: luteinizing hormone supports the production of male sex hormones in the testes and, together with FSH, supports the production of female sex hormones in the ovaries.
Sex hormones
Testosterone in men and estrogens in women are responsible for the development of secondary or secondary sexual characteristics and for behavioral changes.
Testosterone: is a male sex hormone that is produced in the testicles of boys and adult men. Until puberty, his production is low. To a much lesser extent, it is also formed in the gonads of women, where it is a direct precursor and source for the production of female sex hormones.
However, other and much weaker male-acting hormones (androgens) are also produced in the human body in the adrenal glands, which are glands located in close proximity to the kidneys. These hormones affect not only the development of pubic hair (which means hair around the genitals), but also axillary hair (armpit hair) in both boys and girls.
Estrogens: are female sex hormones that affect the development of the breasts and uterus in girls, the place of production is the ovaries. Some androgens are a precursor to the normal production of estrogens in the ovaries. In hormonal disorders of adolescent girls and adult women, their excess may manifest certain symptoms, including menstrual disorders. Lower estrogen levels are also produced in boys by conversion from male sex hormones. In some boys, breast enlargement occurs during adolescence, which usually resolves spontaneously.
Normal puberty (normal adolescence)
Levels of gonadotropins (FSH and LH) and sex hormones are known to be high not only in adolescents but also in normal healthy newborns. This period is also called "mini-puberty". A significant decrease in hormonal levels occurs after 3-6. months. Testosterone levels in boys can be up to half in "mini-puberty" compared to adult men. In the period between 4 and 6 years of age, the production of gonadotropins and sex hormones is very low, with a slight increase occurring in 7-8 years.
Hormonal changes in puberty take place gradually, the development of secondary sexual characteristics begins after reaching the threshold values of hormonal levels. The rise in sex hormone levels begins several years before the development of secondary sexual characteristics.
Puberty is a change in the maturation of the gonads, that is, the testicles in boys and the ovaries in girls. As already mentioned, until puberty, sex hormone levels in boys and girls are very low, their rise affects the development of secondary sexual characteristics and stimulates pubertal growth acceleration. Puberty ends with fertility (sperm production in boys and egg maturation in girls).
Under normal circumstances, puberty in girls begins between the ages of 10 and 13. The first visible manifestation is usually the beginning of the development of the mammary glands and thus the enlargement of the breast, followed by the development of pubic hair. However, it can also be the other way around (the development of pubic hair can precede the development of the mammary glands). The first menstrual bleeding in girls usually occurs between the ages of 11 and 14. The normal range is 10-15 years, most often the first menstrual bleeding (menarche) occurs in our girls aged 12,5-13 years.
In boys with normal sexual development, the testicles enlarge first, then the penis (genitals, genitals) and pubic hair appears. These changes occur between the ages of 10 and 14. Underarm hair, beard growth and deepening of the voice occur in boys typically between the ages of 13 and 16.
The average age of onset of puberty differs by only 6 months for girls and boys, but it can be a difference of several years. This difference may also be related to the well-known experience that early signs of puberty in boys tend to be less noticeable than in girls. Testicular enlargement usually escapes the attention of parents, breast augmentation in girls is obvious and is therefore not overlooked. Although the progression of adolescence is the same for children, the time required for complete maturation ranges from 18 months to 5 years.
Growth acceleration in puberty depends on the production of growth hormone and sex hormones. When one of these hormones fails, the growth spurt is disrupted. In girls, growth accelerates (growth rate - spurt) soon after adolescence, after menarche growth grows. In boys, growth spurt begins later, around mid-puberty.
IF PUBERT APPEARS TO GIRLS BEFORE 8 YEARS AND TO BOYS BEFORE 9 YEAR, IT IS NECESSARY TO SEARCH FOR A SPECIALIST AND TO DETERMINE THE CAUSE OF PRE-ADMINISTRATION. ATTENTION AND THE EXAMINATION DESERVES THE BEGINNING OF PUBERTY IN GIRLS BETWEEN 8.-9. YEAR AU BOY BETWEEN 9.-10. ROKEM.
Glands that control adolescence
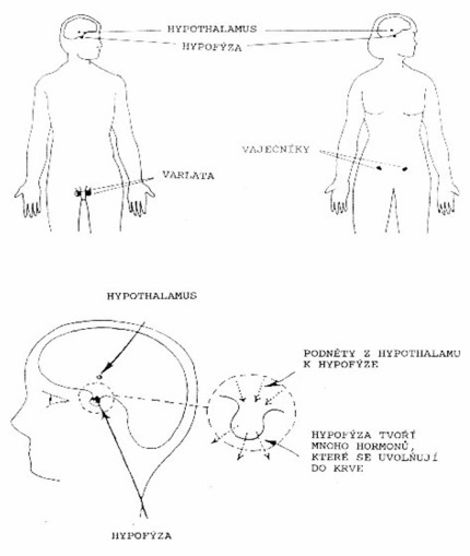
Glands and hormones affecting puberty
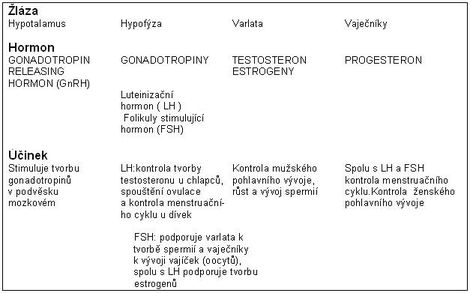
True premature puberty
True precocious puberty may also be referred to as gonadotropin-dependent (ie, gonadotropin-dependent) central precocious puberty. In most cases, it is idiopathic central premature puberty, which means premature adolescence for an unknown cause.
As already mentioned, precocious puberty indicates the onset of adolescence earlier than usual. In true premature puberty, hormonal regulation and the pattern of sexual development coincide with normal puberty, in contrast to the condition referred to as pseudopuberty, which we will discuss elsewhere.
The difference between normal and central premature puberty lies only at the time of onset of puberty.
A premature adolescent may initially be taller and more powerful overall than his or her peers and classmates. Weight gain is associated with premature pubertal growth acceleration (growth spurt). Bone maturation is also accelerated, indicating the biological age of the child (determined from an X-ray of the left wrist and hand). The bone age of the child reflects the prospect of further growth, so we can approximately determine the child's height in adulthood - it is a determination of growth prognosis. Higher growth of a premature adolescent does not mean that this child will be tall in adulthood. Conversely, if treatment is not started in time, growth crevices may close prematurely, growth may stop prematurely, and they may grow smaller than inherited. The goal of treatment is therefore not only to stop premature pubertal development, but also to delay the closure of growth crevices and prolong growth time.
Let us now turn to the other problems that accompany early adolescence. These are changes in the psyche and behavior. These problems do not occur in other children until normal puberty. For example, premature interest in the opposite sex, excitement, self-repentance (masturbation). There are also problems with concentration disorders at school and with integration into the children's team.
In most children, the cause of central precocious puberty is unknown. Activation of the hypothalamic - pituitary - gonadal axis (gonads) and premature male or female sexual development occur earlier than usual. Rarely, cysts or tumors in the lower brain, other diseases of the brain and central nervous system may be the cause of premature adolescence, or they may be a secondary manifestation and consequence of another disease and its treatment. Therefore, in addition to specialist examinations, your pediatrician may also recommend X-rays of the head, CT (computed tomography) or MR (magnetic resonance imaging) to clarify the diagnosis. Brain cysts and tumors causing true premature puberty are more common in boys than in girls, so a detailed examination in boys is always essential. True premature puberty is about 10 times more common in girls than in boys, with late puberty the opposite is true.
Gonadotropin-independent premature puberty
(gonadotropin-independent premature puberty)
This is a premature development of sexual characteristics due to the production of sex hormones, but by a different mechanism than in normal puberty. The cause is a disease of the adrenal glands or gonads (cysts, tumors, a disorder of hormone production in a congenital enzyme disorder). Differentiation is usually possible due to a different order of development of secondary sexual characteristics than in normal puberty (for example, hair development in boys without testicular development). The treatment of these conditions is aimed primarily at eliminating the cause, and thus at eliminating the source of sex hormone production.
Gonadotropin-independent premature puberty occurs in both girls and boys. It may be part of McCune-Albright syndrome (where other endocrine disorders often occur, bone and skin changes may also be present). In a condition called testotoxicosis, the testes develop prematurely, but without concomitant pituitary stimulation, unlike true central premature puberty. This disorder is more common in some families. The treatment is fundamentally different from the treatment of true premature puberty, although the symptoms and course of premature adolescence in testotoxicosis are similar to those in true premature puberty. In boys, premature pseudopuberty may also be due to some hormonally active tumors of the brain, liver, testes and adrenal glands, or it may be a manifestation of increased androgen production in the adrenal glands due to a hormonal disorder. Girls with ovarian cysts, hormonally active adrenal and gonadal tumors may also have premature pseudopuberty, as in boys with hormonal disorders and increased androgen production in the adrenal glands.
Other variants of premature adolescence (incomplete forms)
Premature telarché:
is a trivial and time-bound process. This is a unilateral or bilateral premature breast development. It occurs most often in girls during infancy and can last up to 3-4 years. The onset may be in the first months of life due to maternal hormones that pass into the milk, in which case the telarche usually subsides after breastfeeding. Premature telarche can also occur due to the production of their own ovarian estrogens, either in normal healthy girls with a slower onset of hormonal regulation. Estrogen-producing ovarian cysts have been found in some girls. However, it can also be an increased sensitivity of the mammary glands and breast tissue to estrogens, the levels of which do not exceed normal levels in the body. The possible effect of dietary estrogens is sometimes considered (not clearly established).
At the same time, there are no other manifestations of premature adolescence, the girl's growth is normal.
Breast size may vary (enlarge and shrink) at 4-6 week intervals.
It is necessary to distinguish this insignificant diagnosis from true premature puberty. No treatment is required for premature telarche, only regular monitoring is performed. This condition usually "goes off" within one or two years. Growth and definitive height are not adversely affected. Puberty starts at normal age, fertility is normal. This condition is probably known to many parents because many mild cases do not seek professional examination.
Premature adrenarchy:
is a harmless and time-limited matter. This is the development of pubic hair and / or axillary hair (armpit hair), usually starting between 6-9 years of age, in both boys and girls. Pubic hair here precedes the development of other pubertal features, that is, the development of the penis and testicles in boys and the development of breasts in girls, which starts at the usual age.
There may be a slight acceleration of growth along with a slight and insignificant acceleration of bone age. This is a normal manifestation of adrenal development, the condition requires no treatment, only monitoring.
It is diagnostically important to distinguish this insignificant form of premature adolescence from true premature puberty or from premature pseudopuberty, which may be associated with adrenal cysts or tumors, as previously mentioned. Sometimes a more detailed endocrinological examination (outpatient or short hospital stay) is necessary to clarify the nature of this deviation.
Isolated premature menarche:
These are rare cases of girls who start menstruating before the age of 10 without further signs of sexual maturation. The bleeding can be one-time or repeated at regular intervals for several years and then disappears. At the usual age, normal puberty occurs, including the onset of menstruation. The diagnosis can be made by a specialist only after excluding other causes of premature production of female sex hormones and / or after excluding another cause of vaginal bleeding.
Treatment of premature puberty
A. GnRH analog
(gonadotropin releasing hormone analogues or gonadoliberin analogues) (Decapeptyl depot, Diphereline, Lucrin)
Drugs in this group are chemicals that have some of the natural structure of the gonadoliberin molecule (GnRH). They are designed to block the effect of the naturally occurring hypothalamic hormone gonadoliberin (GnRH). With the help of these drugs, the binding sites in the cerebral cortex (or pituitary gland) for gonadoliberin, which is formed in the body, are occupied. The pituitary gland therefore subsequently reduces the production of gonadotropins (FSH and LH), the stimulation of the gonads decreases until it stops, and the production of sex hormones reaches prepubertal levels. The decline and normalization of hormonal levels is manifested by blocking changes typical of central or true premature puberty. No side effects have been reported with these drugs. Treatment must be carried out without interruption, according to the instructions of a specialist. Discontinuation of treatment leads to support rather than cessation of adolescence. Shortly after starting treatment, before the onset of a beneficial effect of treatment, transient manifestations of mildly progressing puberty may be transient. These include acne, mood swings, a slight increase in breast size, short vaginal bleeding (separating uterine bleeding from a drop in hormonal levels) or rather so-called "spotting". These symptoms disappear within a few weeks of starting treatment. Gonadoliberin analogues are now given in depot (long-acting) intramuscular injections once every 1 days; in some patients, injectable forms that are given once every 28 months can be used. The relevant pediatrician, which is either a pediatric endocrinologist or a pediatric gynecologist, will select the most suitable preparation and method of treatment for your child. Normally, injections are given at 1-day intervals, but may be shorter at the start of treatment. The most suitable treatment cycle is determined for each child by an expert.
B. Cyproterone acetate (Androcur)
This drug acts mainly at the level of the gonads (ovaries and testes), where it prevents the production of male and female sex hormones. It is made as tablets and is usually given 2-3 times a day. In the recent past, its efficacy for the treatment of true (central) puberty has been shown to be insufficient, and thus less suitable than the gonadoliberin analogs mentioned above. Therefore, it has not been used for several years for the treatment of central precocious puberty. An exception may be short-term transient treatment to delay the onset of menarche for various reasons.
Cyproterone acetate is an important drug for another form of precocious puberty that is not dependent on gonadotropins. This drug successfully suppresses the development of premature adolescence, but does not sufficiently reduce the development of bone maturation and therefore does not improve definitive body height.
Cyproterone acetate also affects the production of the adrenal ('stress') hormone cortisol, so adrenal function must be monitored during long-term treatment with higher doses and in some cases cortisol injections must be given to support the body in severe illness or surgery.
C. Other treatment
In some children with a high probability of low adult height, concomitant treatment with a gonadoliberin analogue and growth hormone may be appropriate. These are mainly children with severe growth failure due to intrauterine growth retardation, or children with proven insufficient production of growth hormone. In such cases, delaying the onset of puberty is an advantage, it allows for a prolongation of the growth time (later growth of the growth plates occurs and thus the closure of the growth slits). Research in this area continues.
Social issues
Your child is now probably taller than his peers. It is therefore natural that the environment is considered older. Don't forget his real age and don't overload him with tasks that are excessive for him. Your friends and teachers must also take this into account.
Premature adolescence brings with it a number of social problems. For example, a two-year-old child with premature puberty may look like a five-year-old. However, he has typical behavior for his age, wears diapers, does not completely maintain cleanliness. Mental development corresponds to the actual age of the child, but he looks much older. Premature sexual activity can manifest itself, for example, in erections in boys, masturbating. This attracts the attention and embarrassment of adults. Sweating, acne, and a change in body odor can also manifest as premature adolescence. In that case, we recommend more frequent bathing and washing of hair, skin care.
Children want to look and behave like their peers, and manifestations of premature adolescence often cause confusion and feelings of insecurity. Therefore, it will be very useful to acquaint your child that all girls and boys will go through the same changes, albeit a little later. The child needs to be reassured that the changes related to his body are normal. Allow him to continue his usual activities (sports, hobby groups). However, some of the benefits of accelerated development may be apparent in these activities. Encourage your child to talk about his or her problems. If you think you need help and advice yourself, consult a child psychologist. A specialist will also advise you; the operation of the school can be a partial help.
Even a preventive early intervention by a psychologist can help increase self-confidence and prevent anxiety in later life.
Parents, relatives and others in the area must choose an appropriate attitude towards the adolescent, his problematic behavior, feelings of guilt and mood swings.
Talking to another child's parents with the same problems can be very helpful. As a rule, the family feels alone and completely unprepared for the premature sexual development of the child. Advice and encouragement from other parents or professionals helps the family to guide and cope with the child's difficulties.
Children with early adolescence may also have difficulty with greater physical strength and height. They get into conflicts with their older siblings and parents. Even in this situation, a child psychologist can help.
Frequently asked questions from parents
How do I explain to my child what premature puberty is?
Explain to your child that the changes taking place in his / her body are now normal and that other children will go through them as well, albeit a little later. If you do not know the advice yourself, ask a child psychologist or specialist for advice.
What should we say to friends, relatives, teachers?
Sometimes parents of children do not want their child to have contact with your child. Therefore, it is essential that you explain the nature of premature adolescence and the difficulties associated with such parents. These people do not realize that your child is completely normal, only a teenager earlier. If your child is being treated with injections, you can also explain the effect of this treatment on the temporary cessation of premature puberty.
Behavioral problems can sometimes persist even with successful treatment. We therefore recommend that you ask for the teacher's cooperation. You can contact your specialist who will help you prepare the letter for school.
What will be your height in adulthood?
Body height depends on many circumstances. In conditions such as premature puberty, it is very difficult to determine probable adult height. The height of the parents and the level of the reached biological age play an important role for the child's height (it can be assessed from the ratio between the child's bone age and the actual or calendar age). Accelerating bone age means that the child has less time to grow. In some cases, bone age may be so significantly accelerated that the final height will be significantly reduced. Some girls with premature puberty may have a very mild form of the disease and may reach virtually normal height depending on their genetic base.
Can treatment help control mental balance?
Generally speaking, the answer is yes. Successful treatment is associated with a decrease in sex hormone levels. However, mood swings are not only affected by hormonal levels, they may also be related to a child's response to changes in his or her physique, self-perception, and experiencing differences from other peers. Relationships with other children and adults can also be significant.
A number of other causes can lead to mood swings and unexpected reactions. Clarifying the reasons is important and it is definitely wise not to link all of your child's difficulties only to his or her premature development.
The parents must explain the difference to the younger child from other children in a way that is proportional to his or her mental maturity. Sometimes this can be done with the help of a fictional story, in which we explain the child's problems in an accessible form and help dispel his worries. Sometimes the help of experts is needed, so the family should contact their specialist if they are not able to cope with the situation.
How long will the treatment last?
Hormone suppression treatment for true premature puberty usually lasts until the child reaches the age suitable for puberty. Generally speaking, treatment is usually stopped around the age of XNUMX, the doctor decides on the basis of bone maturity (corresponds to biological age). Calendar and bone age in a child with premature puberty differ from each other. This means that bone age is accelerated compared to calendar age. After treatment, adolescence resumes and progresses at a normal pace. As already mentioned, in conditions with premature pseudopubertia, the treatment is based on the underlying cause and is different from the treatment of central premature puberty.
Does the treatment have any side effects?
Serious side effects in the treatment of true premature puberty with gonadoliberin analogues are unknown. Very rarely, mild headaches may occur temporarily. Treatment of cyproterone acetate in gonadotropin-independent premature puberty can sometimes be associated with fatigue and feelings of exhaustion, which is associated with a decrease in the production of sex hormones and the hormone cortisol in the adrenal glands.
We need to pay close attention to these children. In case of severe illness or surgery, it may sometimes be necessary to inject Hydrocortisone!
Will our adult child have normal fertility?
Experience shows that the treatment of children with premature puberty with gonadoliberin analogues or cyproterone acetate is not an obstacle to normal fertility. In this sense, long-term studies are carried out, the results of which are evaluated on an ongoing basis.
Constipation
Download full text: Constipation [doc; 44 kB]
Download protocol: Protocol - constipation [doc; 28 kB]
Adequate dietary modification will improve intestinal peristalsis and eliminate laxatives in children treated for constipation. Children's diets must contain sufficient ballast substances. These substances are only contained in foods of plant origin!
Ballast substances swell in the intestine, thus increasing the volume of stool, thus supporting the activity of the intestine (its motility-peristalsis) and thus speeding up the intestinal passage (time required for emptying).
Practical advice:
- Foods that support the digestive process (it is recommended to eat them among the main meals) are yoghurts, kefir, sour milk - the bacteria contained in them have a positive effect on the natural intestinal flora and milk sugar has a laxative effect.
- It is recommended to use milk, fruit sugar: add them to dairy products, muesli, fruit drinks
ATTENTION!!! it has a laxative effect but has the same energy. value as normal sugar - To encourage intestinal motility, it is recommended:
- fast in the morning
- drink one glass of water with 1-2 drops of fruit vinegar
- fresh sauerkraut and a little sauerkraut juice
- use "isolated ballast substances" such as wheat bran mix into yogurt, cottage cheese, muesli, cakes, soups, salads or 3 times a day 1-2 tablespoons of bran drink with water. (Wheat bran softens stool, flax seeds have a similar effect). Because these foods swell in the gut, it is necessary to drink 1 glass of liquid for each teaspoon of bran or seeds.
- Gradually introduce foods rich in ballast into the diet (initial bloating can be alleviated by cumin, fennel and anise)
- Sufficient fluids are a must (2-3 liters of fluids a day), fruit and herbal teas, mineral water, fruit juices without sweetening
- Chew every bite enough and allow enough time for each meal
- Eat fresh vegetables or salad prepared from fresh vegetables at least twice a day
The patient should receive plenty of fruits and vegetables. Fruits and vegetables should be fresh and in the form of oil-fortified salads.
Sauerkraut is especially recommended, which, in addition to the mechanical action of ballast substances, affects the intestine by chemical irritation. Lactic acid acts here, which is also contained in other acidic vegetable supplements and in all acidified dairy products.
From acidic dairy products are recommended: milk butter, yogurt, sour milk, skim milk, kefir and more.
Tartaric, malic and citric acids also help to treat intestinal peristalsis. Intestinal peristalsis is treated even after serving roasted coffee beans and drinks rich in carbonic acid.
Due to its thermal effect, the cold drink, which is served on an empty stomach, also has a beneficial effect on intestinal peristalsis.
The administration of nuts and almonds at a dose of 150-200 g / day has a positive effect. However, these foods are not recommended for obese patients due to their high caloric value.
BALASTIC SUBSTANCES ARE CONTAINED ONLY IN FOODS OF THE VEGETABLE NATURE, THEY ARE RECOMMENDED:
- Cereals and wholegrain products - eg cereal grains - in the form of ground mixtures or flakes (eg as muesli), wholemeal bread, meal, flaxseed bread
- Seeds and kernels: flax, sesame and sunflower seeds, pumpkin kernels - softened during the night, for breakfast with muesli or yoghurt, or mixed with sour milk or kefir
- Fruit:
- Dried fruits - raisins, figs, plums, apricots, dates… (possibly soften in water before use)
- Fresh fruit - all kinds except bananas, especially apples and pears (with peel), raspberries, strawberries, currants, gooseberries
- Nuts, almonds: all kinds, !!! rich in calories, with a tendency not to give overweight
- Vegetables: can be served raw (with oil or cream). Sauerkraut, cauliflower and broccoli are especially recommended
- Legumes: Peas, white and dark beans, lentils
- Potatoes: are preferred over rice and pasta
- Sour dairy products: yogurt, kefir, sour or fatty milk are recommended for their stimulating effect on intestinal peristalsis
FOODS THAT ARE NOT RECOMMENDED BECAUSE THE CONTAINMENT WORKS:
- Confectionery - chocolates, pralines, candies, normal sugar and all the foods in which it is contained
- Bread and pastry - white flour products, desserts, cakes, pastries
- Side dishes - paddy rice, pasta
- Desserts - egg flour products
- Drinks - black tea, cocoa, red wine
- Fruit - only bananas and blueberries
NOTE: The diet must be adjusted according to the age of the child. E.g. fluid intake to adapt to the age of the child, for toddlers and smaller children not to give nuts, etc. !!!

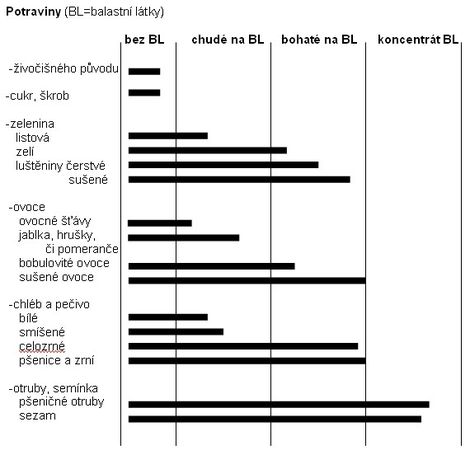
Seminars
Regional seminars
The Pediatric Clinic regularly organizes seminars for primary departments of children's wards and their collaborators. Doctors present interesting case reports, recommended procedures and new trends in treatment.
The directory of regular participants in "primary seminars" has so far been limited mainly to the Central Bohemian Region and Prague. If you are not in the directory as the primary department of the children's ward and you are interested in regular participation, we will be happy to welcome you. Please inform Secretary Bendová (e-mail: helena.bendova@lfmotol.cuni.cz).
The main goal of the Pediatric Clinic of the 2nd Faculty of Medicine of Charles University and the University Hospital in Motol is to provide highly specialized and erudite care to children from all over the Czech Republic.
In almost all areas of pediatrics and adolescent medicine, the Pediatric Clinic has highly qualified specialists - in pediatric nephrology, dialysis and elimination methods, pediatric pneumology, allergology and care for children with cystic fibrosis, pediatric endocrinology and diabetology, pediatric gastroenterology and care. about children with autoimmune diseases. In cooperation with partner workplaces of the Motol University Hospital, we also provide cardiological, immunological and hematological care.
We are ready to help you and your patients whenever you deem it necessary.
Medical seminars of the Pediatric Clinic
Medical seminars of the Pediatric Clinic are held from September to June every Monday, Wednesday and Friday from 7.45 am to 8.30 am in Brdlík's seminar room, entrance through the building of the children's part of the hospital, 1st floor, node D - secretariat. Guests from other workplaces are welcome.
Attendance is recommended for final year students of medical studies.
The current seminar program will be sent to you upon request by the clinic secretary Helena Bendová (helena.bendova@lfmotol.cuni.cz).
Research
List of publications
The list of publications of the staff of the Pediatric Clinic in individual years can be found at https://www.lf2.cuni.cz/info2lf/ustavy/2dk/publik.htm.
Graduate students
MD Katarína Beránková - Early manifestations of bronchial asthma in childhood. Morphological and functional origins of the disease
Field council: Human physiology and pathophysiology
Supervisor: Prof. MUDr. Petr Pohunek, CSc.
MD Jana Djakow - Aspects of identification of patients with primary ciliary dyskinesia
Field council: Human physiology and pathophysiology.
Supervisor: MUDr. Ondřej Cinek, Ph.D., supervisor consultant: Prof. MUDr. Petr Pohunek, CSc.
MD Katarína Mitrová - New regulatory hormones of breast milk
Field board: Biochemistry and pathobiochemistry
Supervisor: MUDr. Jiří Bronský, Ph.D.
MD Lenka Petruželková - Study of first-degree relatives from families of patients with type 1 diabetes mellitus
Field council: Human physiology and pathophysiology
Supervisor: Prof. MUDr. Jan Lebl, CSc., Supervisor consultant: Doc. MUDr. Katerina Stechova, Ph.D.
MD Tereza Ulmannová - Altered gene expression after specific stimulation in first-degree patients with T1D
Field Council: Molecular and Cellular Biology, Genetics and Virology
Supervisor: Doc. MUDr. Katerina Stechova, Ph.D.
M.Sc. Šárka Vošahlíková - Gram-negative pathogens in patients with cystic fibrosis.
Field Council: Molecular and Cellular Biology, Genetics and Virology.
Supervisor: MUDr. Ondrej Cinek, Ph.D.
MD Tomáš Dědic - The role of hereditary factors in the etiology and pathogenesis of childhood cholestatic diseases
Field council: Human physiology and pathophysiology
Supervisor: MUDr. Radana Kotalova, CSc.
Havlišová Magdaléna, MD - Occurrence and importance of secondary ciliary dyskinesia in various types of resorption diseases
Field council: Human physiology and pathophysiology
Supervisor: prof. MUDr. Petr Pohunek, CSc .; MUDr. Jiří Uhlík, Ph.D.
MD Lenka Hoňková - Mechanisms and features of airway wall remodeling in bronchial asthma and other chronic respiratory diseases and their relationship to the course of the disease and changes in respiratory physiology
Field council: Human physiology and pathophysiology
Supervisor: prof. MUDr. Petr Pohunek, CSc.
MD Lucia Karnišová - Hemolytic-uremic syndrome: etiology, genetic profile of patients, identification of other possible pathogenetic factors of the disease
Field council: Human physiology and pathophysiology
Supervisor: doc. MUDr. Kveta Blahova, CSc.
MUDr. Vaclav Koucky - Detection of early changes in lung function in infants and young children with cystic fibrosis, asthma risk and other respiratory diseases
Field council: Human physiology and pathophysiology
Supervisor: prof. MUDr. Petr Pohunek, CSc.
Sage. Lenka Kramná - Picornaviruses in the pathogenesis of islet autoimmunity
Field council: Molecular and cell biology, genetics
Supervisor: Doc. MUDr. Ondrej Cinek, Ph.D.
M.Sc. Jana Matasková - Use of mechanography in the diagnosis of muscle damage in children with chronic diseases
Field council: Human physiology and pathophysiology
Supervisor: doc. MUDr. Zdenek Sumnik, Ph.D.
MD Jan Ohem - Optimization of biological treatment of nonspecific intestinal inflammation (IBD) in children using modern biomarkers
Field board: biochemistry and pathobiochemistry
Supervisor: doc. MUDr. Jiří Bronský, Ph.D.
M.Sc. MD Tomáš Rosík - Proteinuria and its relation to the survival of transplanted kidneys in children
Field council: Human physiology and pathophysiology
Supervisor: prof. MUDr. Tomas Seeman, CSc.
MD Klára Roženková - Influence of mutations in selected genes on beta cell function
Field council: Human physiology and pathophysiology
Supervisor: doc. MUDr. Štěpánka Průhová, Ph.D.
MUDr. Vojtech Sedivy - Influence of perinatal insults on the development of pulmonary vascular circulation
Field council: Human physiology and pathophysiology
Supervisor: prof. MUDr. Jan Herget, DrSc., Prof. MUDr. Vaclav Chaloupecky, CSc.
MD Nadežda Šimánková - BKV polyomavirus in children after kidney transplantation
Field council: Human physiology and pathophysiology
Supervisor: prof. MUDr. Tomas Seeman, CSc.
MUDr. Pera Simunkova - Morphometric and immunohistochemical evaluation of airway wall remodeling in experimentally induced bronchial asthma
Field council: Human physiology and pathophysiology
Supervisor: prof. MUDr. Petr Pohunek, CSc., MD Jiří Uhlík, Ph.D.
M.Sc. Jana Včeláková - Polarization in the direction of Th17 in people really at risk of developing type 1 diabetes
Field council: Immunology
Supervisor: doc. MUDr. Katerina Stechova, Ph.D.
Labs
Laboratory of Molecular Genetics - www.lmg.cz
Laboratory of Autoimmune Diseases - www.labao.cz

Specialization
Dear friends, colleagues, co-workers and sponsors, pediatric patients and their parents!
The Department of Pediatrics of the 2nd Faculty of Medicine of Charles University and the University Hospital in Motol was established in 2004 by merging the work teams of the former I. children's clinic and a significant part of the former II. children's clinic. It is a continuation of their mission - to provide highly specialized and erudite care to children from all over the Czech Republic, whose doctors or parents have requested it. The team of the Pediatric Clinic creates a natural professional background, the "ultimum refugium", for all Czech and Moravian pediatricians, whether they work in children's clinics of teaching hospitals, district children's wards or work as general practitioners for children and adolescents. We are ready to help you and your patients whenever you deem it necessary.
You also meet the staff of the Pediatric Clinic in undergraduate and postgraduate education in pediatrics and its subspecializations, in organizational activities in the care of sick children at the national level and in clinical research and development of biomedical knowledge for the benefit of pediatric patients.
In almost all areas of pediatrics and adolescent medicine, the Pediatric Clinic has highly qualified specialists who provide top diagnostics and therapy - in pediatric nephrology, dialysis and elimination methods, pediatric pneumology and care for children with cystic fibrosis, pediatric endocrinology and diabetology, in pediatric gastroenterology and in the care of children with autoimmune diseases. In cooperation with partner workplaces of the Motol University Hospital, we also provide cardiological, immunological and hematological care.
The credo of the Pediatric Clinic team is "partnership for the benefit of pediatric patients". We are here for you and your patients. Our strength lies in the team experience, in the quality equipment and in the cooperation of the pediatric think tank of the Motol hospital. We strive for straightforward, fast and effective diagnosis and therapy with maximum care for our common pediatric patients.
Our work would be more difficult without sponsors, who make a significant contribution to the renewal and expansion of the clinic's equipment, our "instruments", but also to a friendly and aesthetic environment for our patients. Many thanks to all our sponsors, the clinic team and our patients.
Thanks also go to all Czech and Moravian pediatricians in primary care and inpatient facilities. We highly value their daily endless efforts. It is thanks to them and their work that the sick children who need it most come to us. We thank them for recommending and sending these patients to us. I am sure that it is through our joint efforts that we achieve the maximum possible for the well-being of sick children.
Prof. MD Jan Lebl, CSc.,
on behalf of the team of doctors and nurses of the Pediatric Clinic
Contact
Address:
V Úvalu 84
150 06, Prague 5
Knowledge:
head - Prof. MUDr. Zdenek Sumnik, Ph.D.
Chief Medical Officer – primary doc. MD Štěpánka Průhová, Ph.D.
head nurse - Mgr. Jana Boháčová, phone: +420 22443 2005
Secretariat:
Medical Secretariat
Jana Šašková, phone: +420 22443 2002
Lenka Viktorinová, phone: +420 22443 2004
School secretariat
Klára Borecká, phone: +420 22443 2001
fax: + 420 22443 2020
Email: pediatrie@fnmotol.cz, pediatrie@lfmotol.cuni.cz
Contact with health insurance companies
Jitka Doubravová
phone: 224 432 007
Email: jitka.doubravova@fnmotol.cz
Workplace
| cardiology outpatient clinic - ECG | 6th floor Polyclinic | 224 432 073 |
| nephrology clinic | S1. floor B - bed part | 224 432 080, 2086 |
| diabetological outpatient clinic | 1th floor Polyclinic | 224 433 813, 3811 |
| endocrinology clinic | 1th floor Polyclinic | 224 433 813, 3811 |
| gastroenterological outpatient clinic | 1th floor Polyclinic | 224 432 031, 2013 |
| anthropology | 1th floor Polyclinic | 224 432 260 |
| pneumological outpatient clinic | 1th floor Polyclinic | 224 432 012 |
| cystic fibrosis center | SP. floor Polyclinic | 224 432 227, 2230 |
| examination of chlorides in sweat | 1th floor Polyclinic | 224 432 272, 2067 |
| spirometry | 1th floor Polyclinic | 224 432 265, 2067 |
| obesitology | 1th floor Polyclinic | 224 433 821 |
| pediatrics | 1th floor Polyclinic | 224 432 042, 2044, 3812 |
| pediatrics - nurse | 1th floor Polyclinic | 224 433 816 |
| comprehensive care center | 1th floor Polyclinic | 224 433 790 |
| gastroenterology department | P. floor A - bed part | 224 432 011, 2039 |
| infant ward | P. floor C - bed part | 224 432 033 |
| nephrology department | 1st floor C - bed part | 224 432 234, 2240 |
| Department of Diabetology and Endocrinology | 1st floor B - bed part | 224 432 010, 2029 |
| Department of Pneumology and Allergology | 1st floor A - bed part | 224 432 207, 2032 |
| Intensive Care Unit | P. floor B - bed part | 224 432 238, 2278, 2208 |